Download to read offline





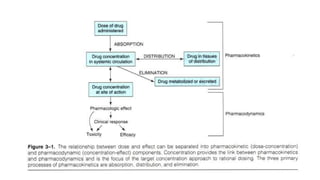























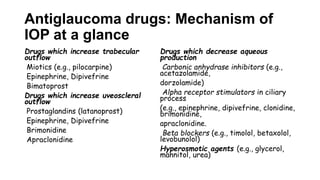








This document outlines various topics related to ocular pharmacology including general pharmacological principles, diagnostic drugs, therapeutic drugs, adverse drug effects, pharmacokinetics, pharmacodynamics, drug classifications, modes of ocular drug administration, ocular anesthesia, common antimicrobial agents, and more. It provides information on drugs used for conditions like glaucoma, uveitis, infections and inflammation.





















































































