Downloaded 437 times
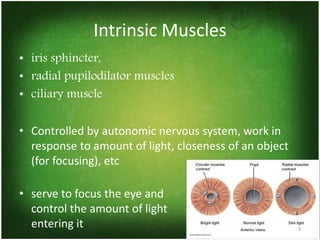
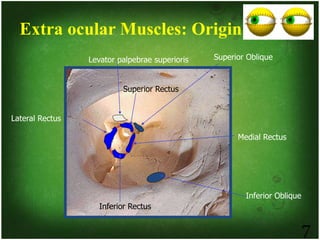
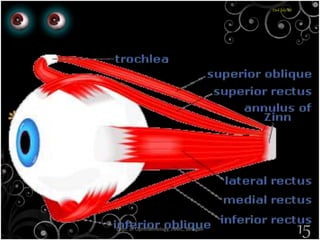
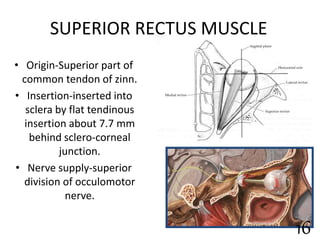
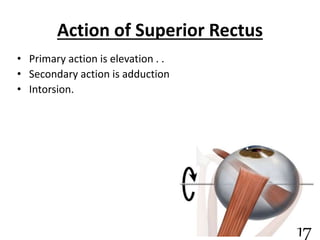
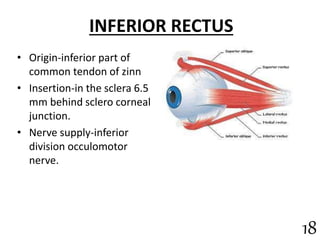
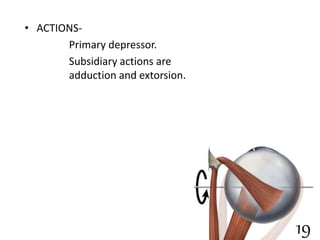
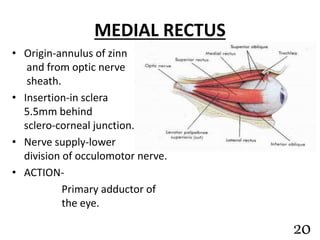
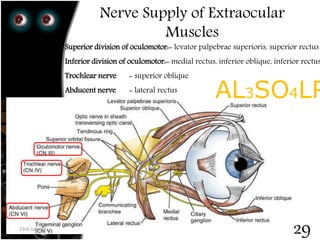
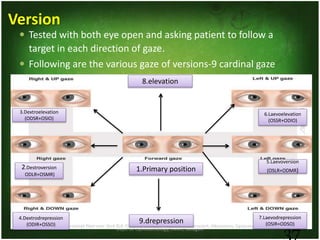
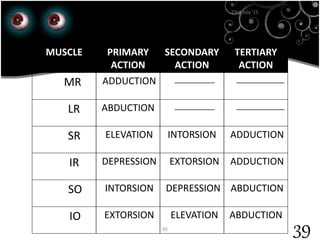
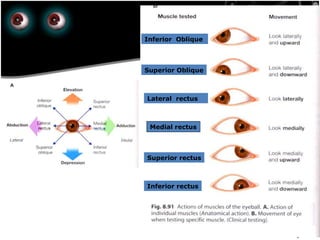
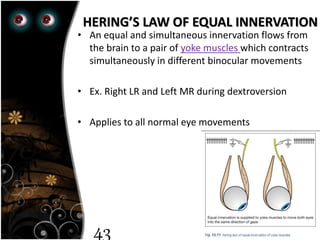
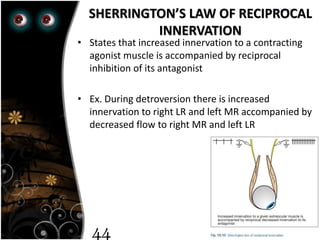


The document describes the extra-ocular muscles that control eye movement and pupil size. It discusses both the intrinsic muscles that control the lens and pupil, and the extrinsic muscles involved in eye movement. The six extrinsic muscles include the superior, inferior, medial, and lateral rectus muscles, and the superior and inferior oblique muscles. Each muscle is described in terms of its origin, insertion, nerve supply, and primary action. The document also covers ocular movements including versions, ductions, and vergences. Laws of ocular motility like Hering's law of equal innervation are also summarized.























































































