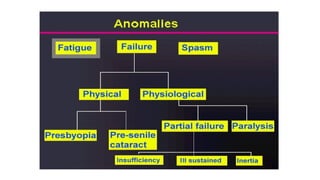



This document discusses various anomalies of accommodation that can occur, including accommodative fatigue, presbyopia, insufficiency of accommodation, inertia of accommodation, paralysis of accommodation, and spasm of accommodation. It describes the symptoms, causes, assessments, and management approaches for each condition. The key message is that anomalies of accommodation are common and their management is an important part of optometric practice.




















































































