The document summarizes key anatomical and physiological details of the extraocular muscles and eye movements:
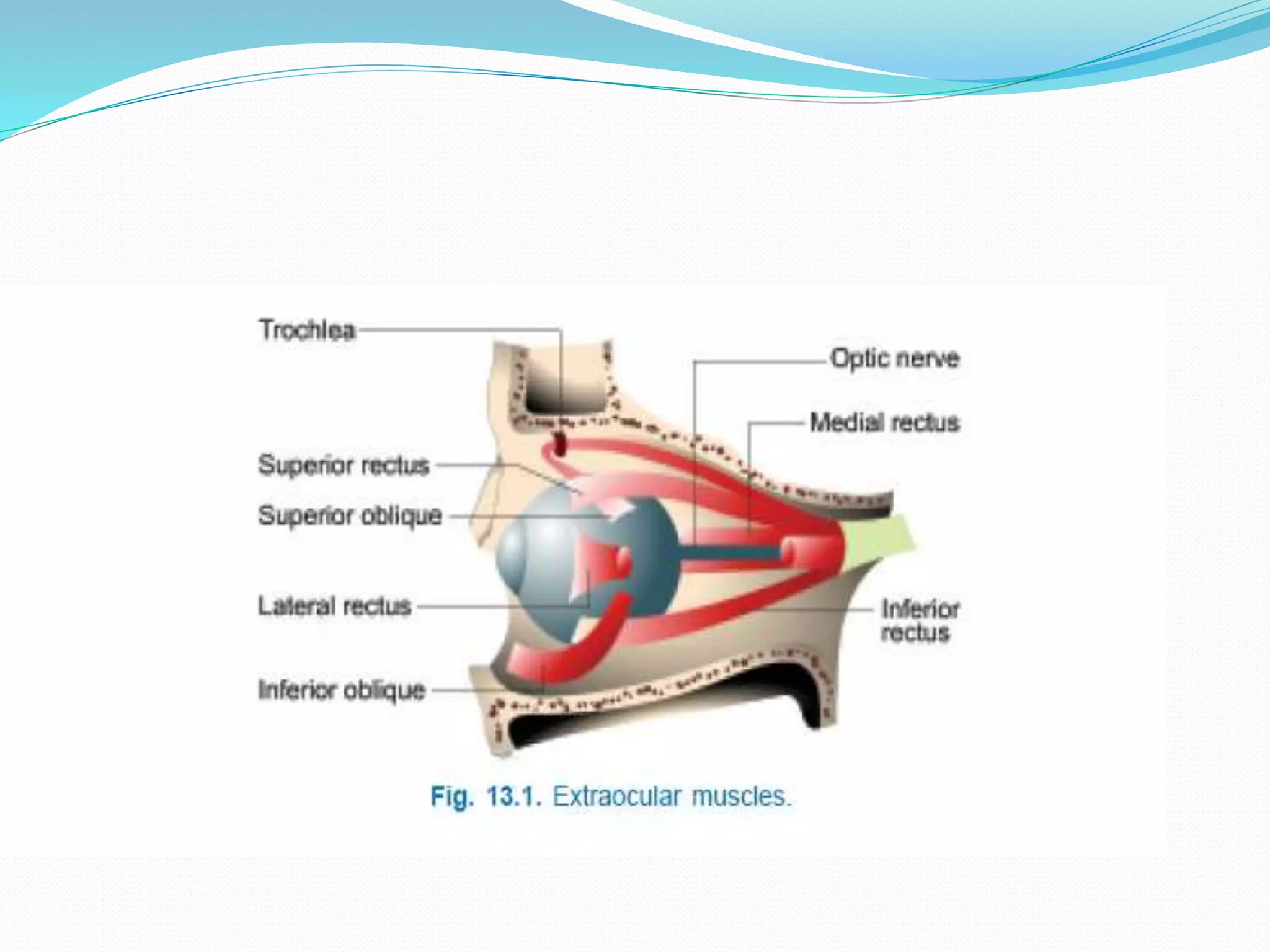
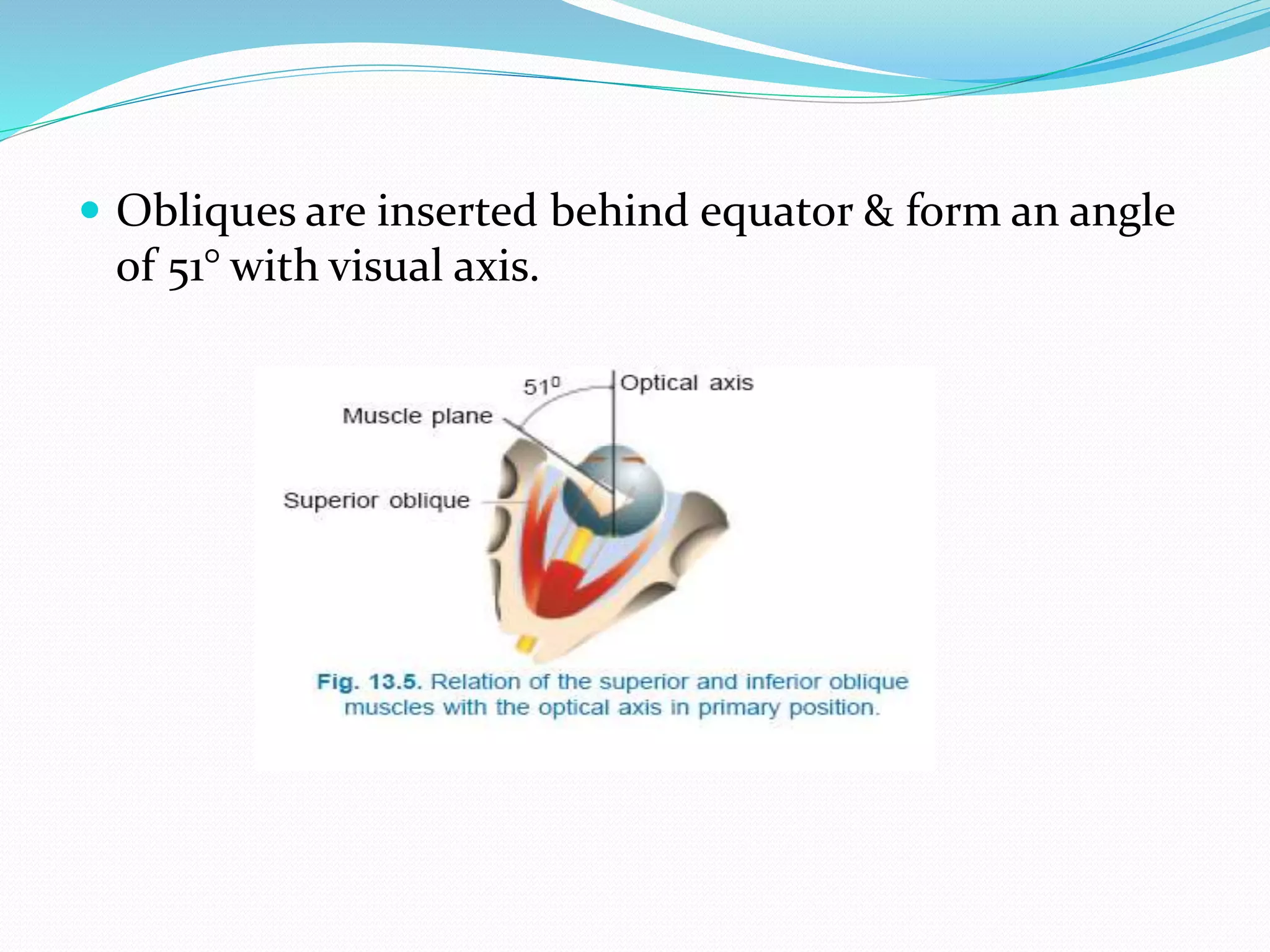
1. It describes the bony orbit anatomy, six extraocular muscles and their actions, innervation and blood supply. The four rectus muscles control horizontal and vertical eye movements, while the two oblique muscles enable torsional movements.
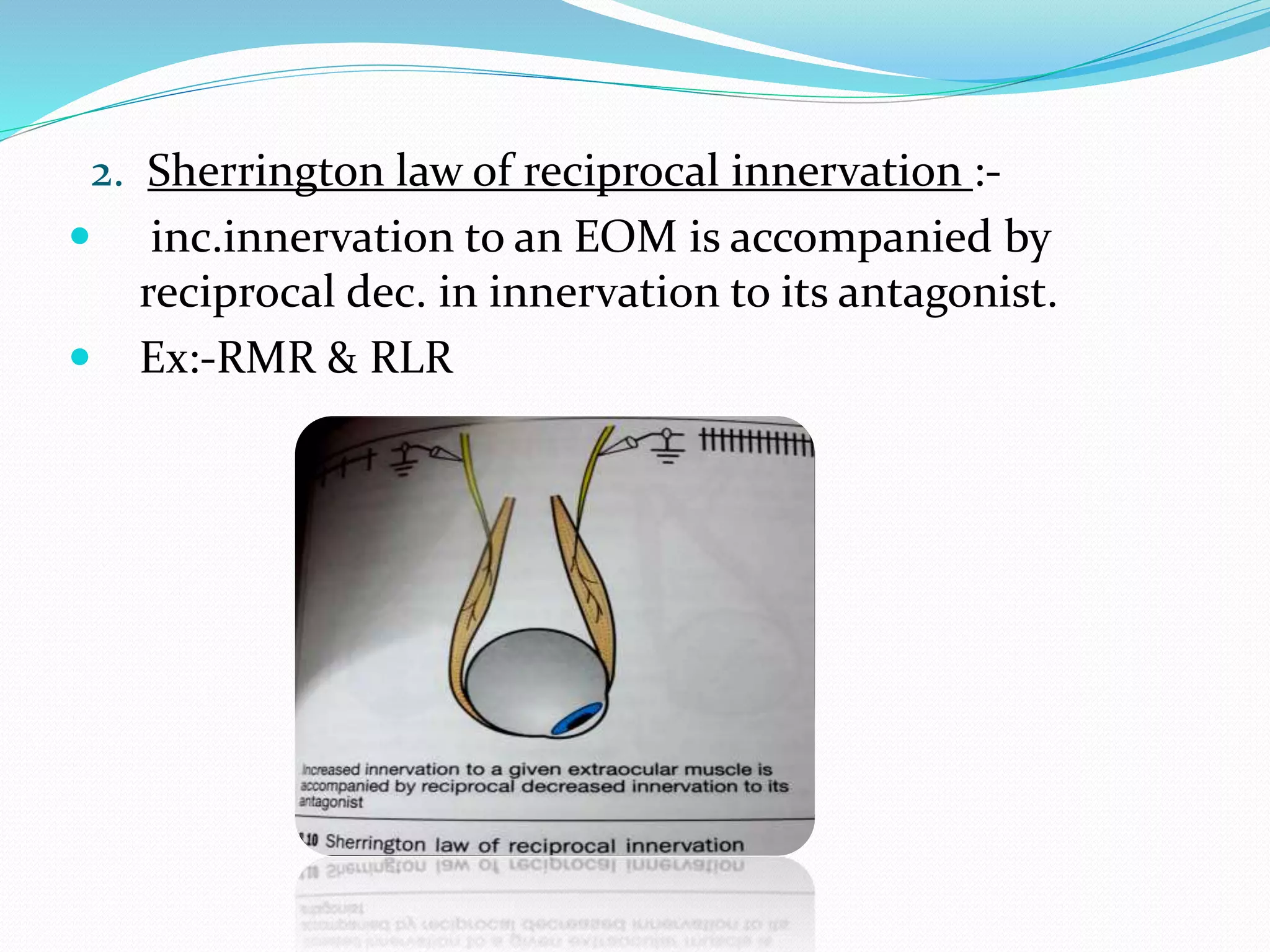
2. The document outlines uniocular and binocular eye movements including versions, vergences, and diagnostic positions of gaze. Hering's and Sherrington's laws govern coordinated eye movements between the eyes.
3. Supranuclear control systems like saccadic, smooth pursuit, vergence and vestibulo-ocular pathways mediate voluntary and reflexive eye movements