Downloaded 778 times
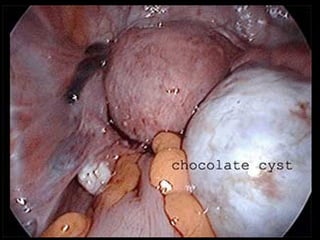
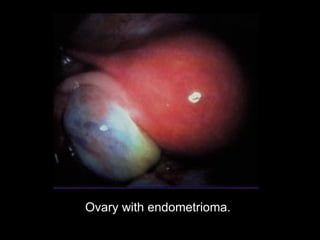
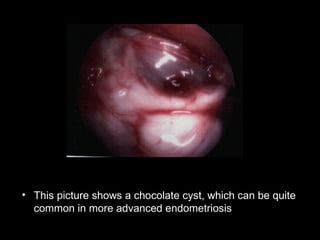
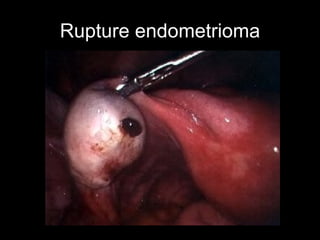
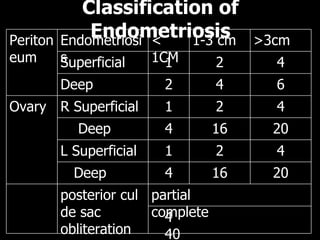



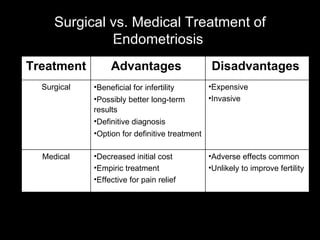
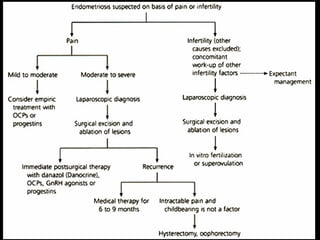

Endometriosis is characterized by the presence of endometrial tissue outside the uterus, commonly causing pelvic pain and infertility. It is a progressive disease that is diagnosed via laparoscopy. Treatment options include hormone therapy, surgery, or a combination, with the goal of relieving symptoms and potentially improving fertility. Recurrence rates after surgery are estimated to be around 19% after 5 years but are lower with more extensive surgical intervention such as oophorectomy.











































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)