Downloaded 44 times

![HISTORICAL BACKGROUND
• Characteristics of disease described at least as far back as 1600 BCE
• Schrön described a “female disorder in which ulcers appear[ed] in the
abdominal, the bladder, intestines and outside the uterus and cervix,
causing adhesions”
• First histological description credited to Von Rokitansky
• Cullen later suggested endometriomas (“adenomyomas”) resembled
mucous membrane of uterus
• Sampson generally credited for providing first theory on pathogenesis;
coined term “endometriosis” in 1921](https://image.slidesharecdn.com/endometriosis-170711173627/85/Endometriosis-3-320.jpg)

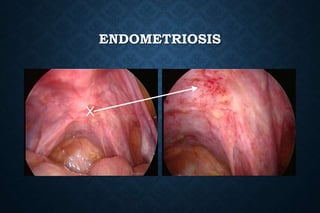




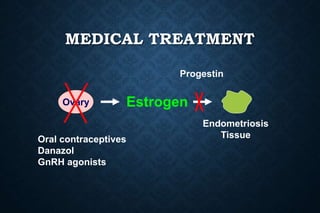
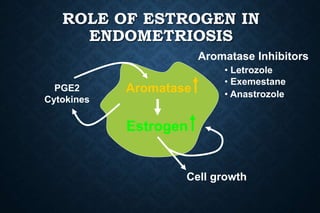
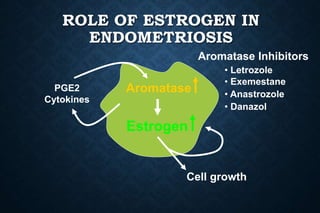


Endometriosis is a disease where endometrial tissue grows outside the uterus, most commonly in the pelvis. It can cause pelvic pain, infertility, and other symptoms. Treatment involves surgery to remove lesions and adhesions, as well as medical therapy using hormones to suppress ovarian function and estrogen production. Newer medical treatments targeting aromatase and local estrogen production are also showing promise for reducing endometriosis-associated pain.





































![Endometriosis Disease by Slidesgo[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/endometriosisdiseasebyslidesgo1-241101144133-f0bd970b-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
