Downloaded 1,044 times






















![Uterine arterial embolization in the treatment of adenomyosis UAE procedures were performed in 23 patients with adenomyosis. After treatment the symptoms and uterine volume of all patients were investigated. All clinical symptoms of 23 patients relieved. Dysmenorrhea completely disappeared in 19 patients, significantly alleviated in 2 patients. But in other 2 recurred. The uterine volume shrunk significantly [(50 +/- 18)%] vs [(100 +/- 0)%]. The blood flow within the uterine and lesions detect by color doppler flow imaging decreased immediately after UAE. Low-abdominal pain and slight fever were seen after treatment and recovered within 1 - 2 weeks. Chen C, Liu P, Lu J, Yu L, Ma B, Wang J, Liu P Zhonghua Fu Chan Ke Za Zhi 2002 Feb; 37 :77-9](https://image.slidesharecdn.com/adenomyosis245/85/adenomyosis-51-320.jpg)



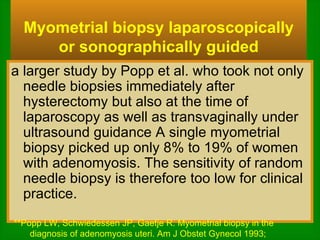
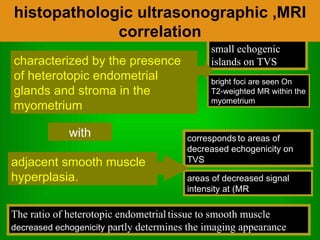
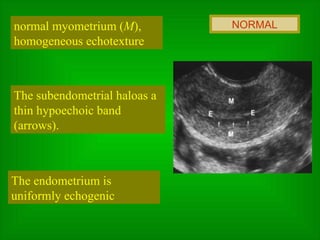
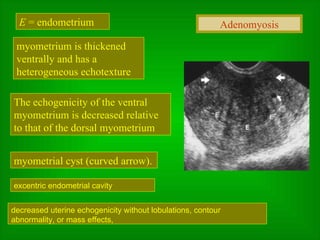
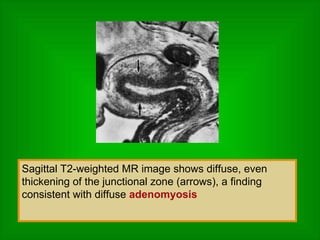
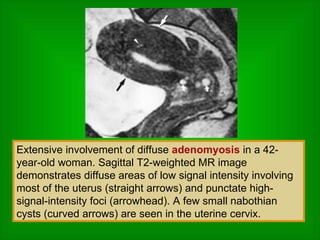
The document discusses adenomyosis, a benign condition where endometrial tissue grows within the uterine wall. It defines adenomyosis and describes associated symptoms like pelvic pain and abnormal bleeding. Diagnosis can only be confirmed by pathology after hysterectomy, though other imaging methods like ultrasound and MRI can provide clues. TVUS shows heterogeneous myometrial texture while MRI may detect increased thickness or consistency changes in the myometrium.



































































