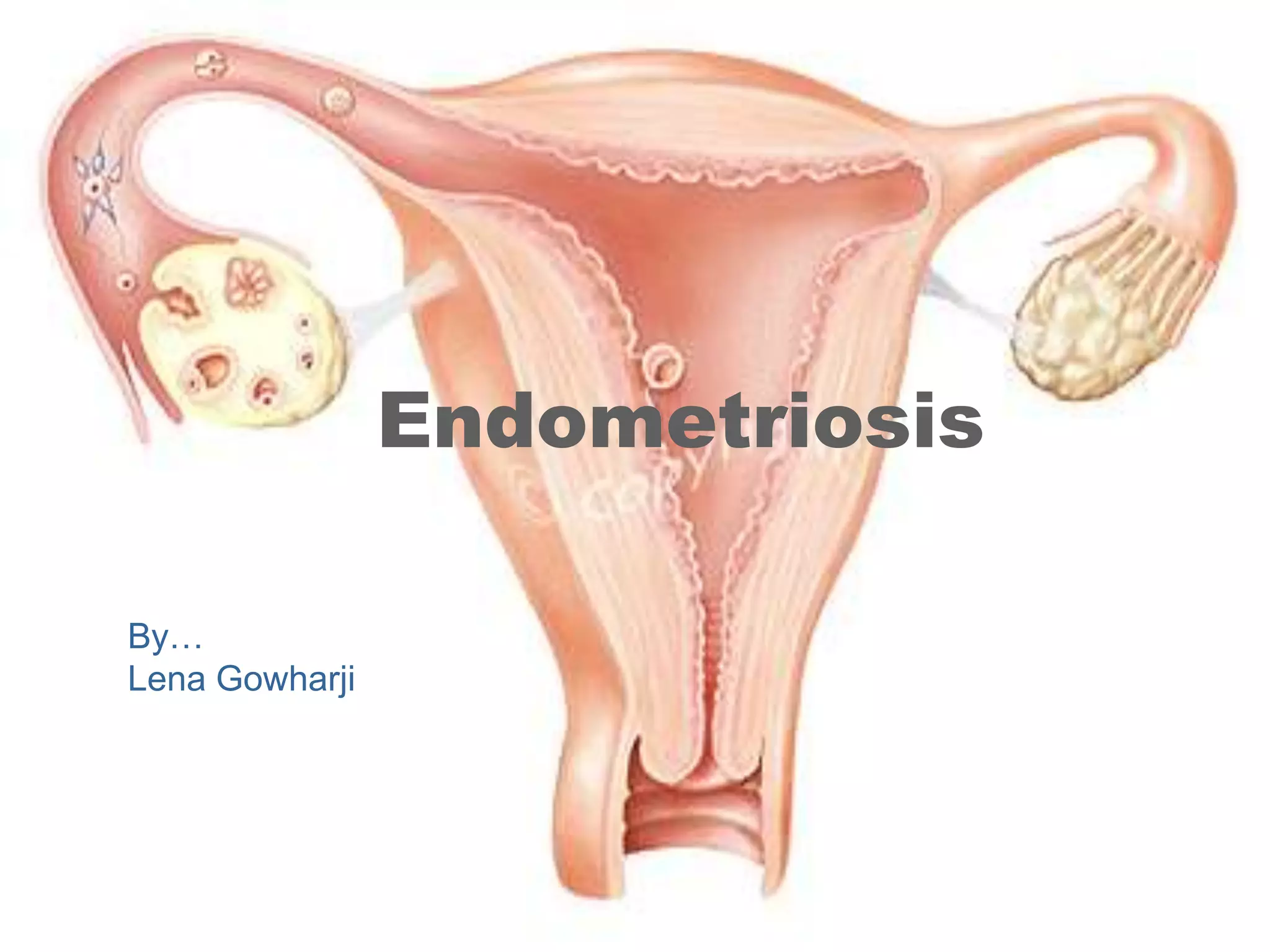
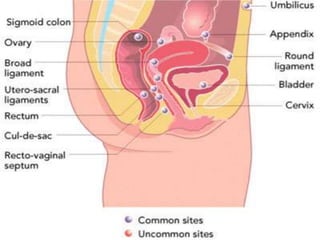
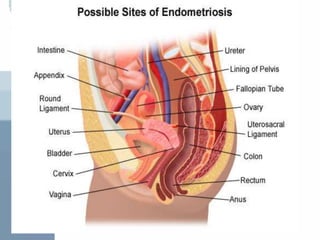
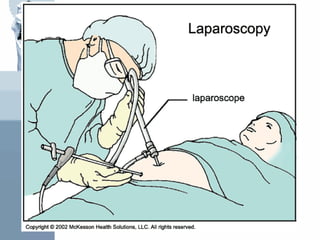
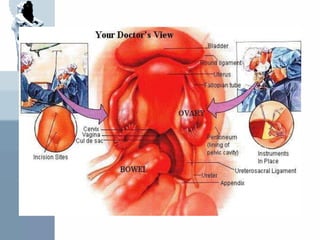
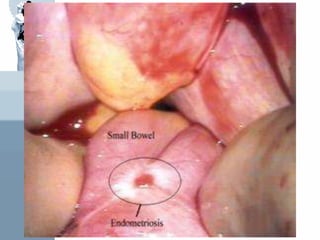
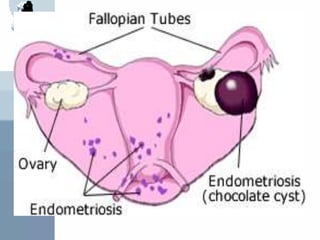
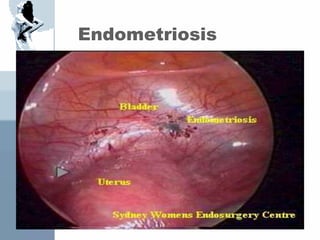
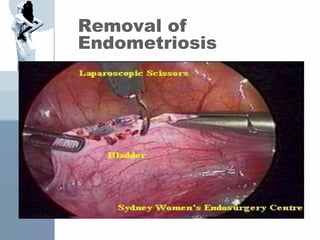
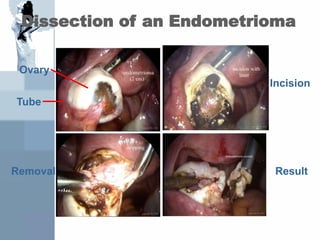
Endometriosis is a condition where endometrial tissue grows outside the uterus, most commonly on the ovaries, ligaments and peritoneal surfaces in the pelvis. It causes painful periods, pain with intercourse, and infertility. While the exact cause is unknown, retrograde menstruation is a leading theory. Diagnosis requires laparoscopy and biopsy of lesions. Treatment involves pain medication, hormonal therapy to induce a pseudo-menopause or pregnancy state, or surgery to remove the lesions. Conservative surgery aims to remove mild disease while radical surgery involving a hysterectomy and bilateral oophorectomy is used for severe cases.









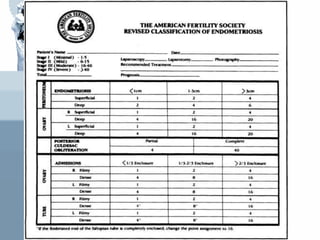
![If the fimbriated end of fallopian tube is completely
enclosed, change the point assignment to 16
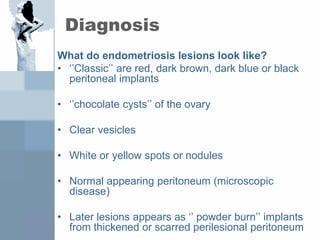
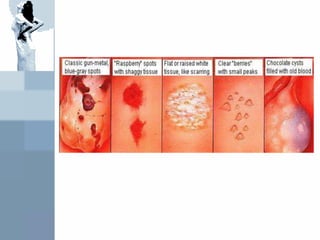
Denote appearance of superficial implant type as
RED [(R), red, red-pink, flamelike, vesicular
blobs, clear vesicles]
WHITE [(W), opicifications, peritoneal defect,
yellow-brown]
BLACK [(B), black, hemosiderin deposits, blue]
Denote % of total described as R__%, W__%,
B__%](https://image.slidesharecdn.com/bayerendometriosis-230928065225-5ae0286d/85/bayer-endometriosis-ppt-41-320.jpg)













































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






