Download as PDF, PPTX
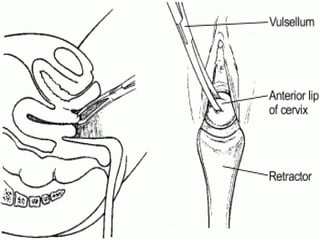
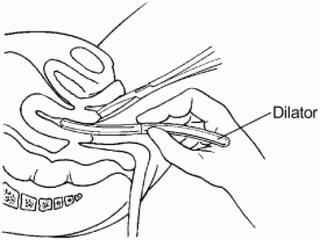
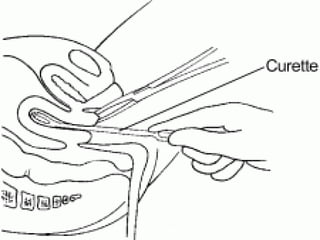
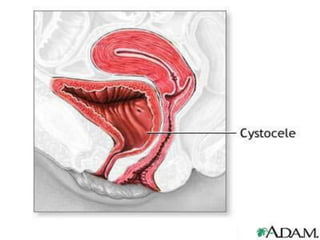
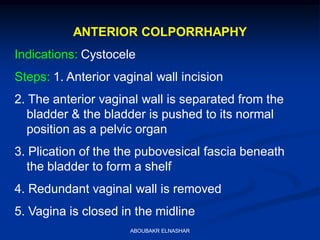
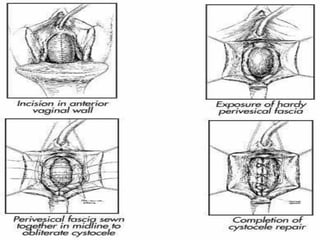
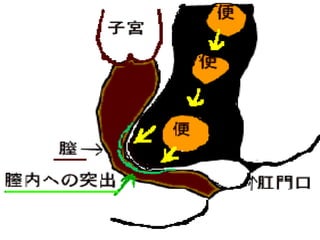
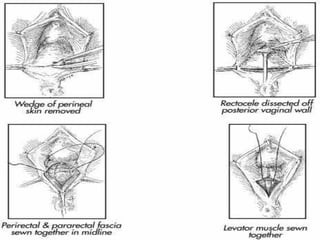

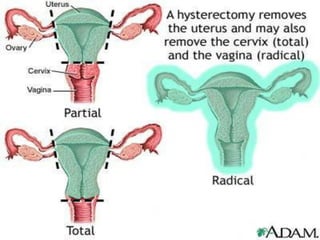



The document discusses various gynecological procedures including: 1. Dilatation and curettage which is used to dilate the cervix for procedures like hysteroscopy or IUD insertion and to curette the uterine cavity to diagnose or treat conditions. 2. Anterior and posterior colporrhaphy which are used to repair cystocele and rectocele by incising and suturing the anterior and posterior vaginal walls. 3. Fothergill's operation which is used to treat combined vaginal and uterine prolapse and involves cervical amputation and shortening of ligaments. 4. Various myomectomy and hysterectomy techniques for removing fibroids and





































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





