Definition
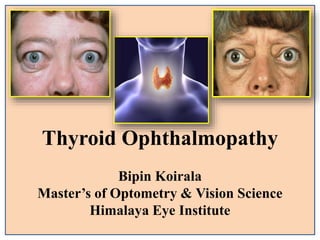
Thyroid eye disease(TED) is an autoimmune disease
caused by the activation of orbital fibroblasts by
autoantibodies directed against thyroid receptors.
TED is a rare disease, which had an incidence rate of
approximately 19 in 100,000 people per year .
4.
Introduction
These changes havealso been called as :
Endocrine Exophthalmos
Malignant Exophthalmos
Dysthyroid Ophthalmopathy
Ocular Graves’ Disease (OGD)
Thyroid Eye Disease (TED)
5.
Introduction
Incidence of ThyroidEye Disease depending on thyroid
disorder
Hyperthyroidism-90%
Primary hypothyroidism-1%
Hashimoto thyroiditis-3%
Euthyroid -6%
6.
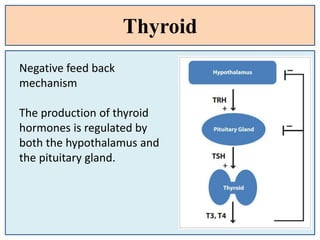
Thyroid gland
Location: Anteriorneck beneath the larynx
Endocrine gland and highly vascular and supplied by
autonomic nervous system.
Has over a million follicles that secrete thyroglobulin, a
precursor of the thyroid hormones, On activation the
thyroglobulin is re-absorbed, converted into the
thyroid hormones triiodothyronine (T3) and thyroxine
(T4),
Hyper Thyroid
Hyperthyroidism isa condition that results from an over-
secretion of thyroid hormones.
It is usually caused by an autoimmune disease known as
Graves’ disease,
Common causes :
Thyroiditis
Toxic adenomas,
Toxic nodular/ multinodular goiters
Thyroxine overdoses
Excess iodine dietary intake.
9.
Hypo Thyroid
Hypothyroidism isdue to an underactive thyroid gland and
results in a deficiency of thyroid hormones.
Thyroid hormones are essential for normal development
between birth and puberty and a deficiency causes
irreversible mental retardation.
Hypothyroidism can be caused by Hashimoto’s thyroidism,
Pathophysiology
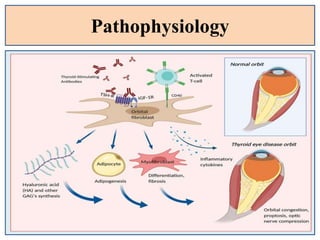
TED being anautoimmune disease with orbital fibroblast as the
primary target inflammatory attack and the EOM are secondarily
involved
Also the target antigen is shared b/w thyroid follicular cells and
orbital fibroblast
The activated T cells acts on fibroblast – adipocyte lineage with in
orbit and will stimulate adipogenesis, fibroblast proliferation and
GAG synthesis as a result of which EOM are enlarged due to
infiltration and odema
13.
Pathophysiology
There is anincrease in the volume of the orbital contents,
particularly the muscles, which can swell to eight times their
normal size.
There may be a secondary elevation of intraorbital pressure, and
the optic nerve may be compressed.
Later muscle fibres eventually leads to fibrosis, which exerts a
tethering effect on the involved muscle, resulting in restrictive
myopathy and diplopia
Common Risk Factors
Female(4-6 times) and middle aged
Smoking (no of cigarettes per day)
H/O auto immune thyroid disorder
HLA-DR3 and HLA-B8 positive
Genetic predispsition
Life style
16.
Symptoms : Ocular
Dryeyes
Ocular redness and irritation
Reduced vision
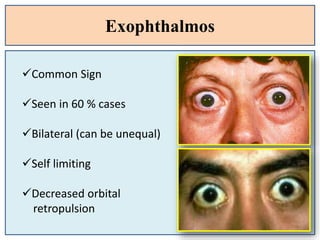
Bulged eye
Diplopia
Eyelid odema
Pain and pressure around eye
Field loss
Dyschromatopsia
17.
Clinical features (lidsigns)
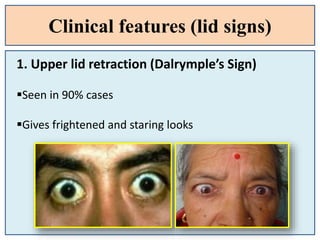
1. Upper lid retraction (Dalrymple’s Sign)
Seen in 90% cases
Gives frightened and staring looks
18.
Clinical features (lidsigns)
G
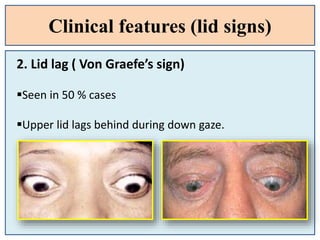
2. Lid lag ( Von Graefe’s sign)
Seen in 50 % cases
Upper lid lags behind during down gaze.
19.
Clinical features (lidsigns)
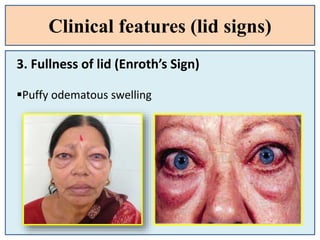
3. Fullness of lid (Enroth’s Sign)
Puffy odematous swelling
20.
Clinical features (lidsigns)
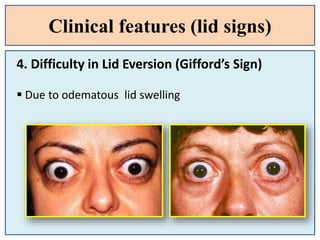
4. Difficulty in Lid Eversion (Gifford’s Sign)
Due to odematous lid swelling
21.
Clinical features (lidsigns)
4. Infrequent / Incomplete blinking
(Stellwag’s Sign)
5. Presence of Glabellar furrow’s
22.
Clinical Features (LidSigns)
1. Rosenbach's Sign: Fine tremors of the eyelids when closed.
2. Boston’s Sign: Jerky irregular movement of upper lid on
downward gaze.
3. Kocher’s Sign: Increased lid retraction with visual fixation
4. Abadie Sign: Spasm of the levator palpebrae superioris
muscle with retraction of the upper lid.
5. Riesman's sign: Bruit heard over the closed eye with a
stethoscope.
Clinical features (Pupil)
Inequality of dilation of pupil
Other Pupillary Signs:
1. Cowen’s Sign: Jerky pupillary constriction to
light.
2. Lowy’s Sign: Mydriasis with instillation of lower
concentration of adrenaline.
3. Knies’s sign: Unequal dilatation of pupil in dim
light.
25.
Clinical features (EOM)
1.Möbius Sign: Inability to converge.
2. Ballet Sign: Restriction of one or more
extraocular muscles. (40 %)
3. Jendrassik's Sign: Limitation of abduction and
rotation of eyeballs.
4. Suker’s Sign: Poor fixation on abduction.
26.
Clinical features (EOM)
Question1:
What is the most commonly and initially
affected EOM??
Answer:
Inferior Rectus (Elevation defect is seen)
Medial Rectus ( Defective abduction)
@ IMSL
27.
Clinical features (Facial)
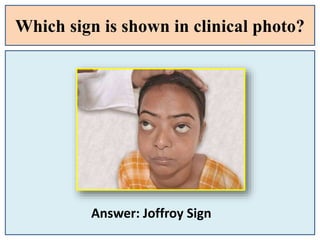
1.Joffroy Sign: Absent creases in the forehead on
superior gaze.
2. Jellinek's Sign: Hyperpigmentation of the superior
eye folds.
3. Hertoge’s Sign: Loss of the lateral third of eyebrows
4. Sainton’s sign: Delayed forehead wrinkling on up
gaze.
28.
Which sign isshown in clinical photo?
Answer: Joffroy Sign
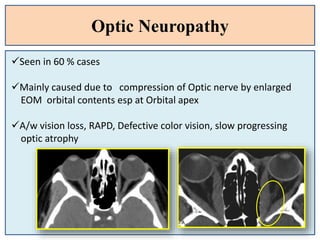
Optic Neuropathy
Seen in60 % cases
Mainly caused due to compression of Optic nerve by enlarged
EOM orbital contents esp at Orbital apex
A/w vision loss, RAPD, Defective color vision, slow progressing
optic atrophy
33.
Rare Associations
Strabismus dueto muscle fibrosis
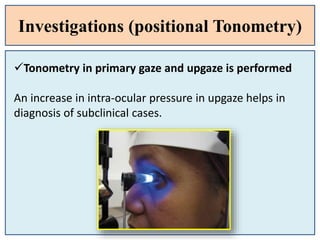
Glaucoma
Raised IOP in up gaze
Increased Episcleral Venous pressure
Increased Mucopolysaccharide deposit with in Aq. Outflow
system
34.
Differential Diagnosis
Orbital orPreseptal cellulitis
Carotid-cavernous fistula
Idiopathic orbital inflammation (Pseudotumour)
TED must be ruled out in all cases of B/L proptosis
35.
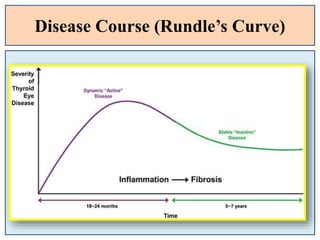
Disease Course andPhases
The pattern of the disease follow the Rundle’s curve which
describe the plot of orbital disease severity against time
1.Initial phase- inflammatory phase duration may last from 6 –
18 months with orbital and periorbital signs i.e. proptosis and
retraction.
2.Static phase- decrease in the inflammatory phase and
minimal improvement.
3.Quiescent phase- gradual improvement with improved
motility and retraction of the muscles
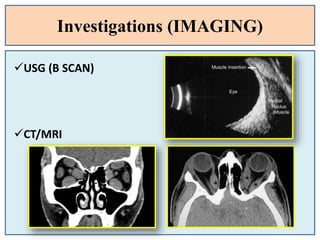
Investigations (IMAGING)
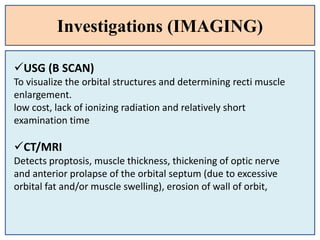
USG (BSCAN)
To visualize the orbital structures and determining recti muscle
enlargement.
low cost, lack of ionizing radiation and relatively short
examination time
CT/MRI
Detects proptosis, muscle thickness, thickening of optic nerve
and anterior prolapse of the orbital septum (due to excessive
orbital fat and/or muscle swelling), erosion of wall of orbit,
Basic Investigations
1. Correctedvisual acuity and Refraction
2. Color vision testing
3. Examination for an afferent pupillary defect
4. Extraocular muscle motility examination
5. Measurement of the lid fissure height in primary
gaze
46.
Basic Investigations
1. Measurementof upper and lower scleral show,
2. Exophthalmometry to detect proptosis
3. Slit-lamp biomicroscopy to assess the tear film and
fluorescein pattern
4. Fundus examination to detect optic disc swelling or
pallor.
47.
Treatment
Treatment can beclassified into that of
1. Mild disease (most patients),
2. Moderate to severe active disease,
3. Post inflammatory complications.
4. The first measure taken in all cases should be the
cessation of smoking.
5. Thyroid dysfunction should also be managed
adequately
48.
Treatment (Mild disease)
1.Topical artificial tear drops in the day time and
ointment at bed time are useful for relief of ocular
surface drying
2. Head elevation with three pillows during sleep to
reduce periorbital oedema.
3. Eyelid taping during sleep may alleviate mild
exposure keratopathy.
4. Oral NSAIDs may be used for periocular pain.
49.
Treatment (Optometry pointof view)
1. For diplopia, Fresnel prisms or occlusion therapy
may be considered.
2. Prism for restricted ocular motility
3. Base in prism for reduced convergence
4. Others are lifestyle modifications e.g. sodium
restriction to reduce water retention and tissue
edema
50.
Treatment (Moderate toSevere disease)
1. Guanethidine 5% eyedrops may decrease the lid
retraction caused by overaction of Muller’s muscle.
2. Systemic steroids may be indicated in acutely
inflamed orbit with rapidly progressive chemosis
and proptosis with or without optic neuropathy
3. Radiotherapy (2000 rads given over 10 days period).
It may help in reducing orbital oedema in patients
where steroids are contraindicated
51.
Treatment (Moderate toSevere disease)
5. Lateral tarsorrhaphy
Performed in patients with exposure keratopathy (with
mild to moderate proptosis) not responding to topical
artificial tears
6. Extraocular muscle surgery.
It should be carried out for left-out diplopia in primary
gaze, after the congestive phase of disease is over and
the angle of deviation is constant for the last 6
months.
52.
Treatment (Post complications)
7.Orbital wall decompression
It involves the orbital floor, medial wall, and lateral
wall. In rare cases the roof of the orbit may also be
decompressed surgically.
53.
PATIENT’S DETAIL
• Name:SHANTI SHARMA
• Age: 33 years Sex: Female
• Occupation: House wife
• Mode Of Presentation :
Regular eye checkup
56
HISTORY OF PRESENTILLNESS
• No h/o of eyeball pain
• No h/o of photophobia
• No h/o of diplopia or polyopia and shadowing of
objects (ghost image)
• No h/o of itching of eye(s)
58
56.
PAST- OCULAR HISTORY
•H/O using glasses since 1 year with
Rx
OD: -0.50 Dsph with 6/6̊
OS: - 0.50 Dsph with 6/6̊
• No other h/o of past ocular diseases and surgery
• Using tear substitute for past 1 yr
59
57.
PAST- SYSTEMIC HISTORY
•No h/o of Diabetes Mellitus / Hypertension
• H/0 hypothyroidism +
• No h/o of surgical intervention for any disease
• No h/o of any other systemic illness in past
• h/o of use of systemic medication for hypothyroidism for 6 months
• Tab. Thyronorm 25 mcg - OD
60
58.
PERSONAL HISTORY
• Nonvegetarian by diet
• Does not consume alcohol and smoke
• House wife by proffesion
61
59.
FAMILY HISTORY
• Noany systemic and ocular diseases in other family
members
• No family members being syndromic or with inherited
abnormalities
60 65
33 25
62
60.
General Physical Examination
•Average built, well nourished
• Weight – 54kg Height – 1.5m BMI - (21.10kg/m2)
Vitals
• Blood Pressure = 120/80 mmHg (Left arm, sitting position)
• Pulse = 82 beats per min, regular.
• Respiration rate= 18/min, regular
• Temperature: 98.6⁰F
General Examination
• No pallor, icterus, clubbing, cyanosis, lymphadenopathy or
edema. 63
61.
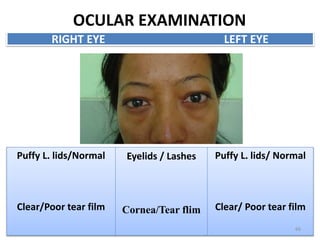
OCULAR EXAMINATION
On theday of presentation:
RE VISUAL ACUITY LE
6/9 p UNAIDED 6/9 p
6/6 AIDED 6/6
6/6 PH 6/6
64
OCULAR EXAMINATION
Puffy L.lids/Normal
Clear/Poor tear film
Eyelids / Lashes
Cornea/Tear flim
Puffy L. lids/ Normal
Clear/ Poor tear film
RIGHT EYE LEFT EYE
66
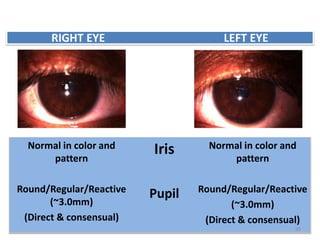
Normal in colorand
pattern
Round/Regular/Reactive
(~3.0mm)
(Direct & consensual)
Iris
Pupil
Normal in color and
pattern
Round/Regular/Reactive
(~3.0mm)
(Direct & consensual)
RIGHT EYE LEFT EYE
69
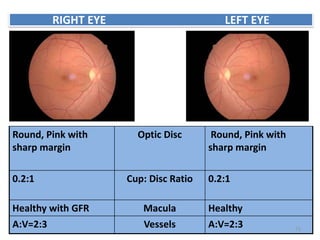
Round, Pink with
sharpmargin
Optic Disc Round, Pink with
sharp margin
0.2:1 Cup: Disc Ratio 0.2:1
Healthy with GFR Macula Healthy
A:V=2:3 Vessels A:V=2:3
RIGHT EYE LEFT EYE
71
69.
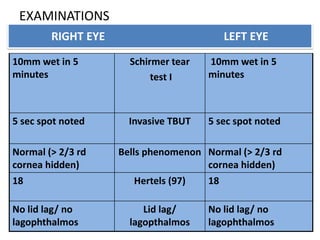
EXAMINATIONS
10mm wet in5
minutes
Schirmer tear
test I
10mm wet in 5
minutes
5 sec spot noted Invasive TBUT 5 sec spot noted
Normal (> 2/3 rd
cornea hidden)
Bells phenomenon Normal (> 2/3 rd
cornea hidden)
18 Hertels (97) 18
No lid lag/ no
lagophthalmos
Lid lag/
lagopthalmos
No lid lag/ no
lagophthalmos
RIGHT EYE LEFT EYE
#19 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#20 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#21 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#22 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#23 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#24 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#25 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#26 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#27 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#28 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#29 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#30 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#31 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#32 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#33 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#34 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#35 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#36 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#37 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.
#38 The most common cause of unilateral or bilateral upper eyelid retraction is Graves’ ophthalmopathy, or thyroid eye disease. Early in Graves’ disease, eyelid malposition may result from increased sympathetic activity. With time, the levator palpebrae superioris and Müller’s muscle become hypertrophic, fibrotic, and adherent to orbital tissues. Patients with thyroid eye disease often have associated globe proptosis and lid lag along with eyelid retraction. Lower lid retraction is usually not seen in patients with Graves’ ophthalmopathy without concomitant retraction of the upper lids. Upper eyelid retraction in thyroid eye disease often has temporal flare, when retraction is more pronounced at the lateral aspect of the eyelid.