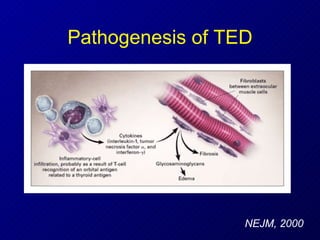
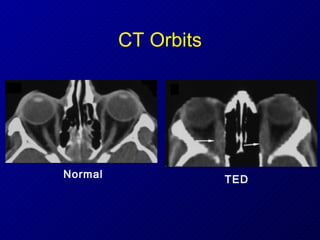
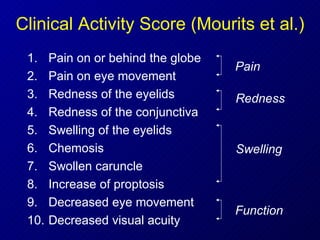
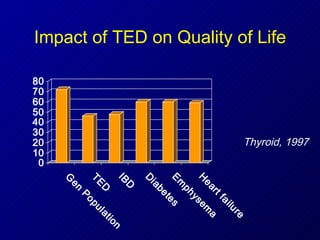
1) Thyroid eye disease (TED) is an autoimmune disorder associated with Graves' disease. It can affect the eye muscles, fatty tissue, and optic nerve.
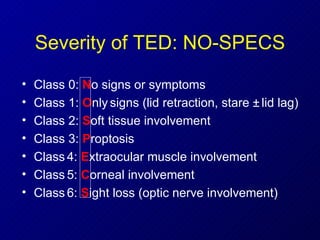
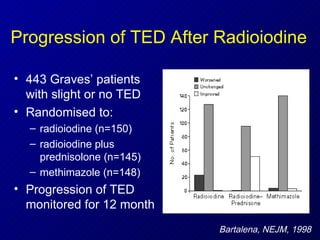
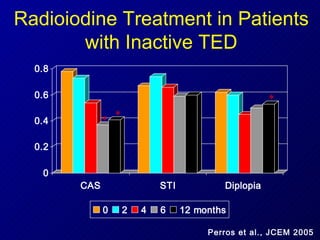
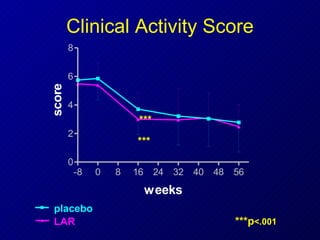
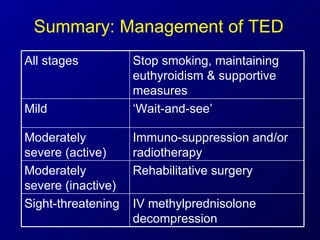
2) Treatment depends on the severity and activity of TED. Mild and inactive cases may only require monitoring. Moderate to severe active TED is treated with intravenous steroids, radiation therapy, or surgery. Sight-threatening TED urgently requires treatments like steroids and orbital decompression.
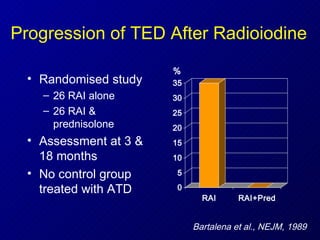
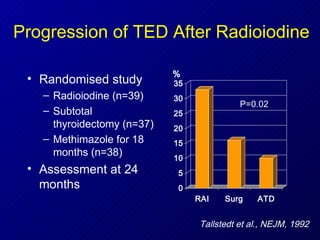
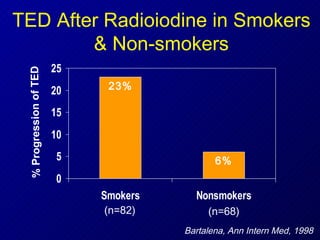
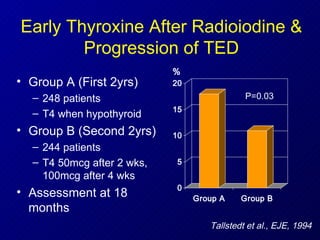
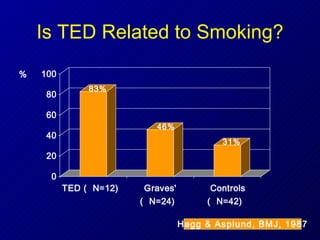
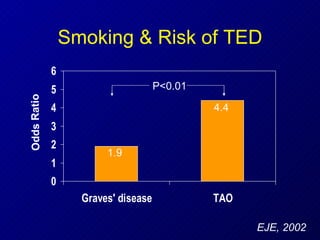
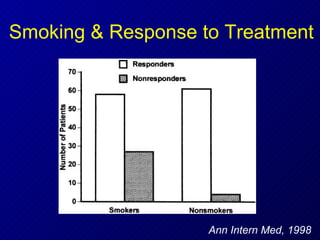
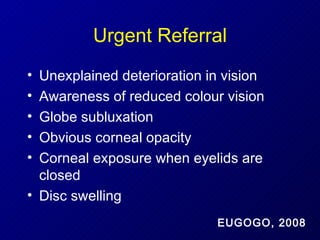
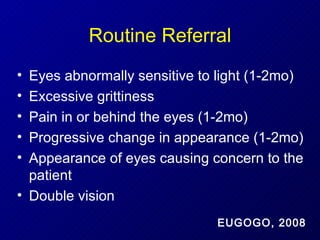
3) Managing thyroid function and advising patients to stop smoking can help prevent progression of TED. Referral to a specialist TED clinic is recommended for persistent or worsening eye symptoms.























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

