Downloaded 455 times





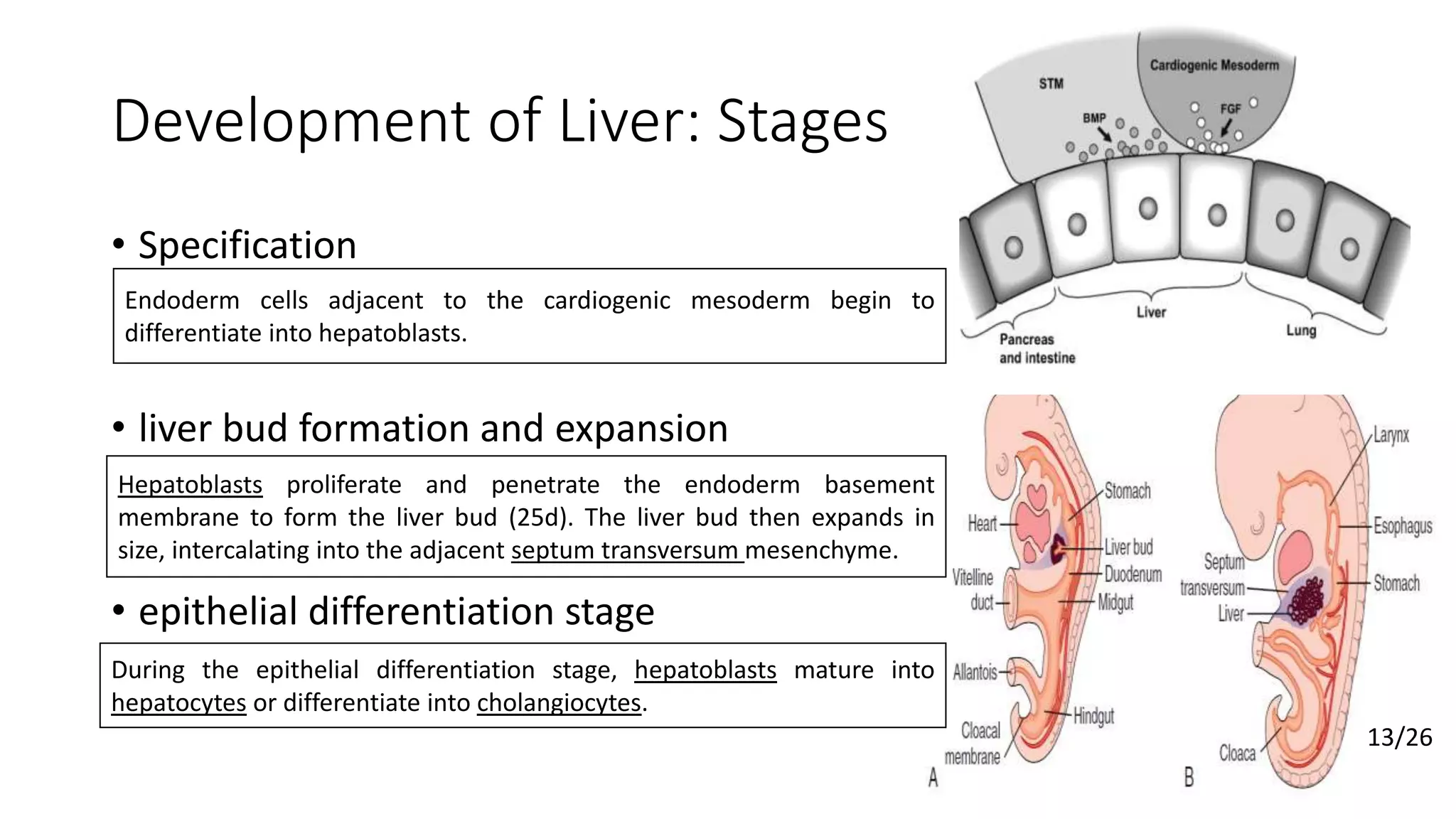
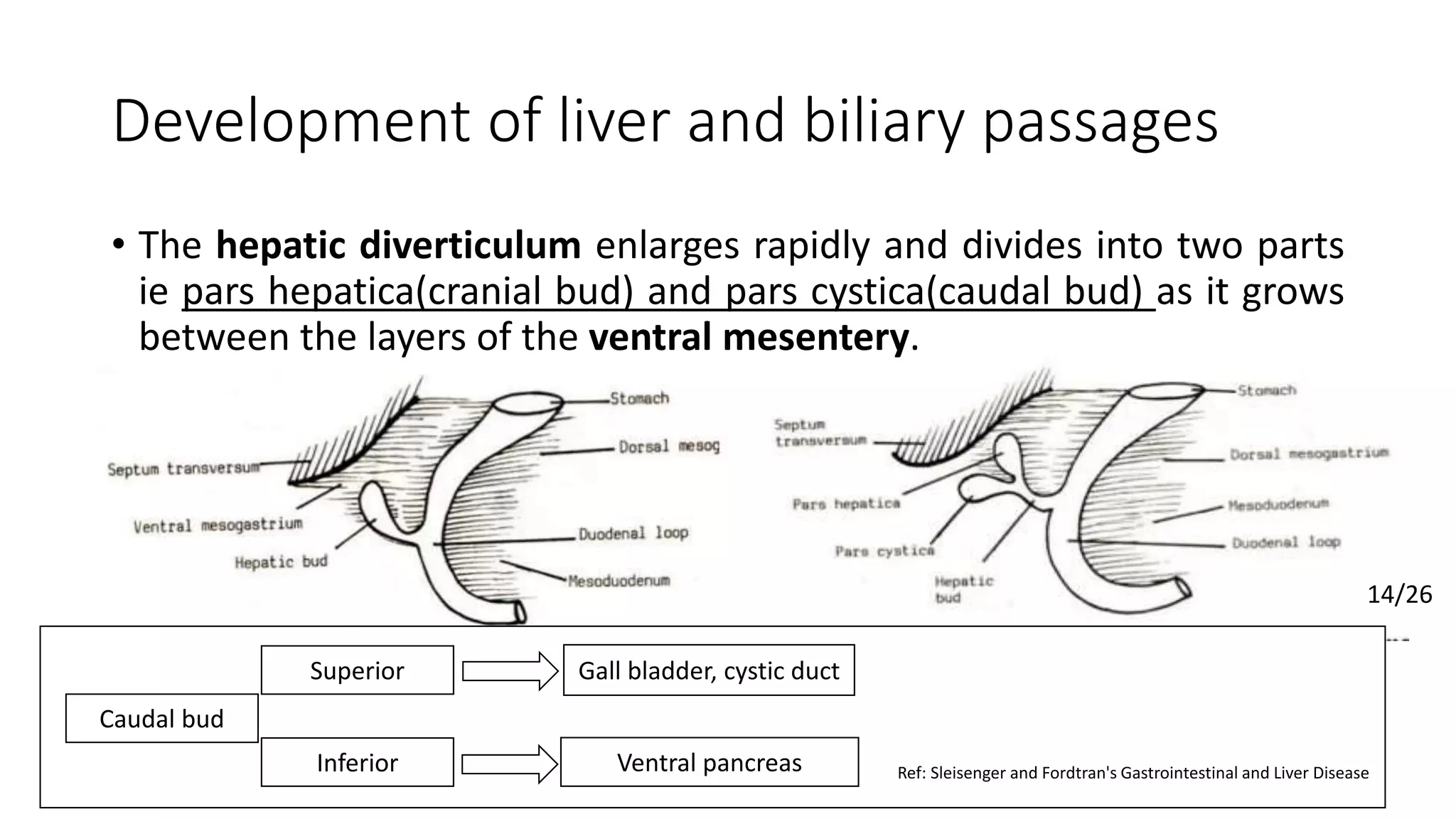

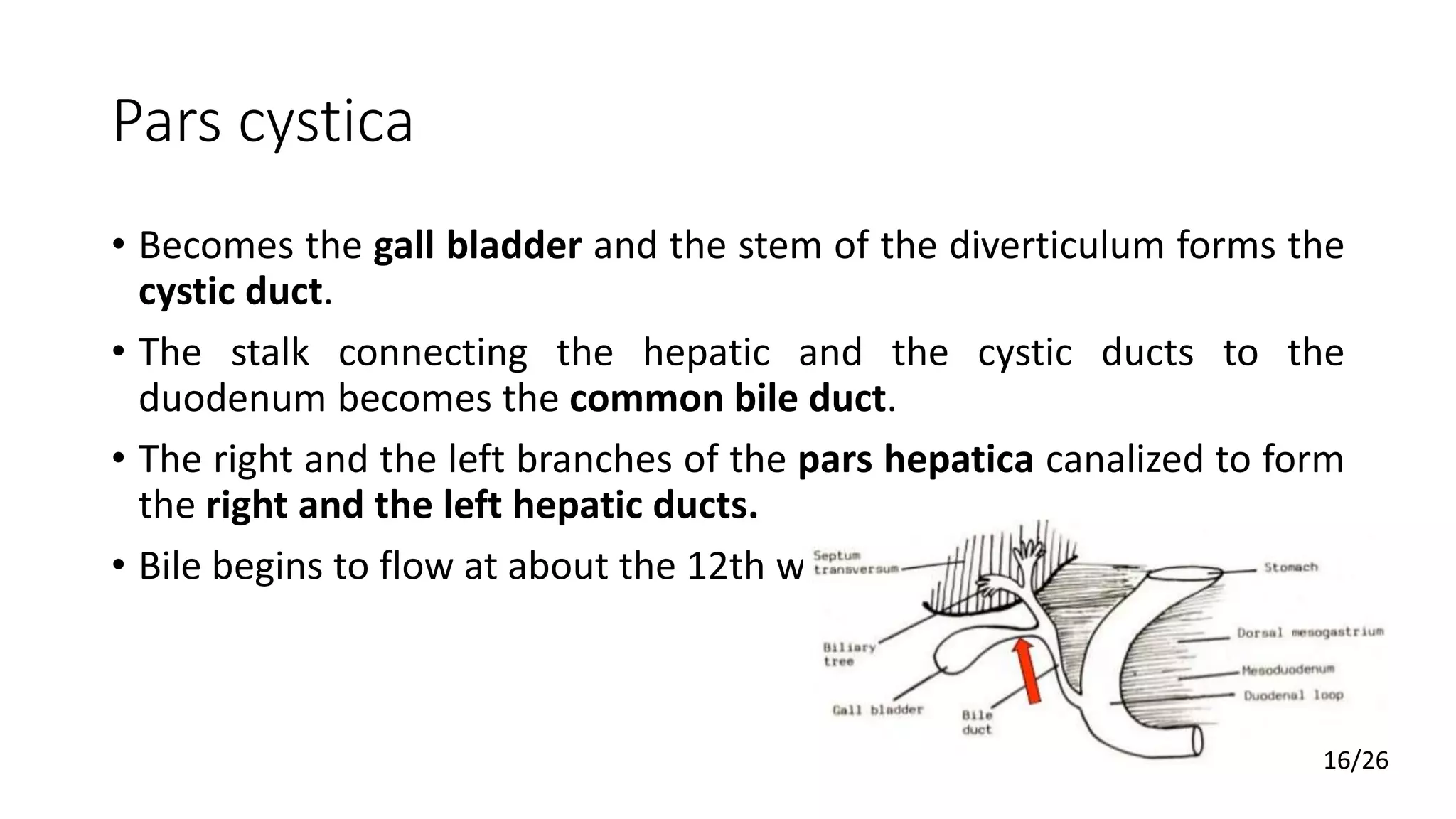
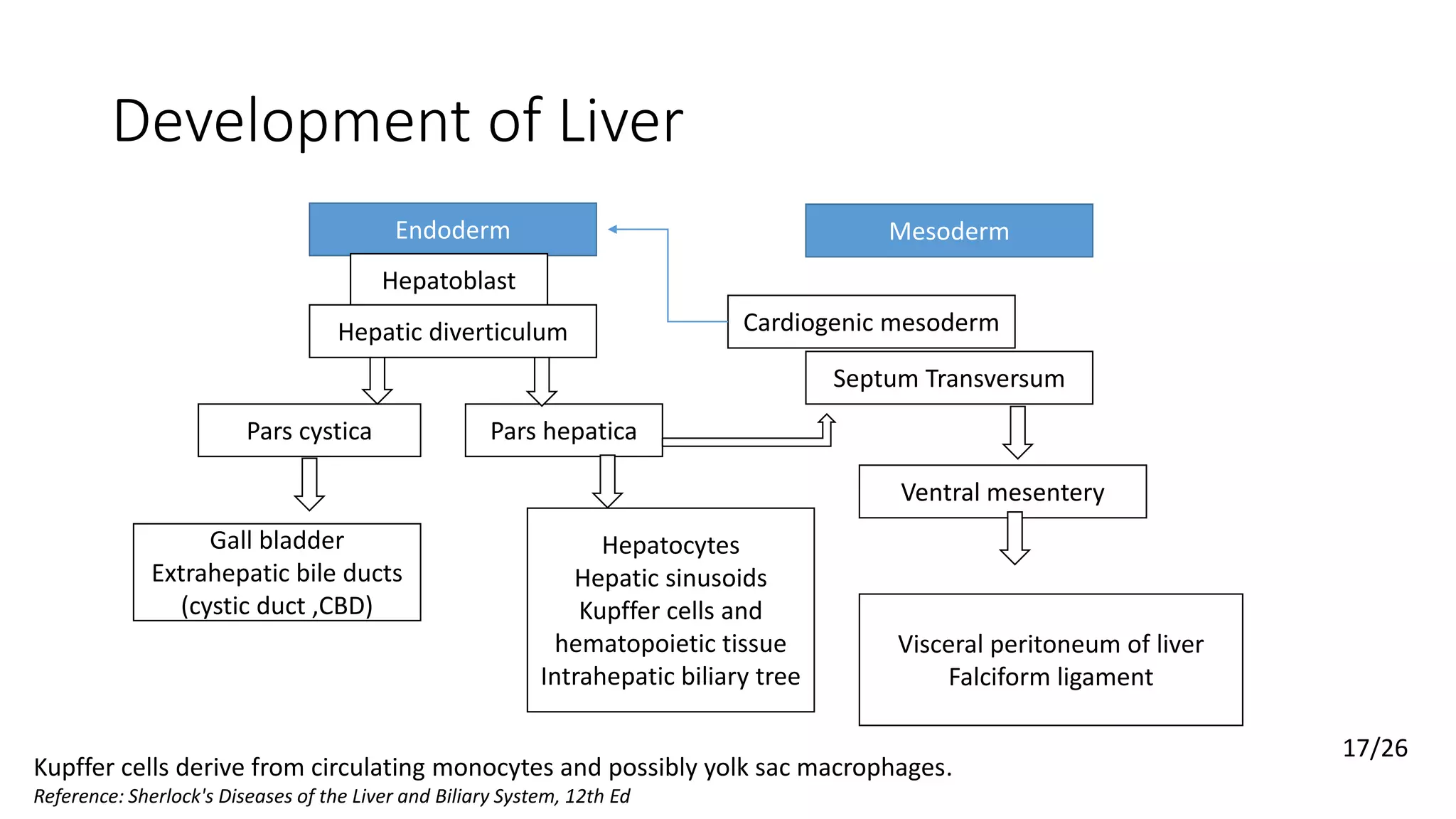
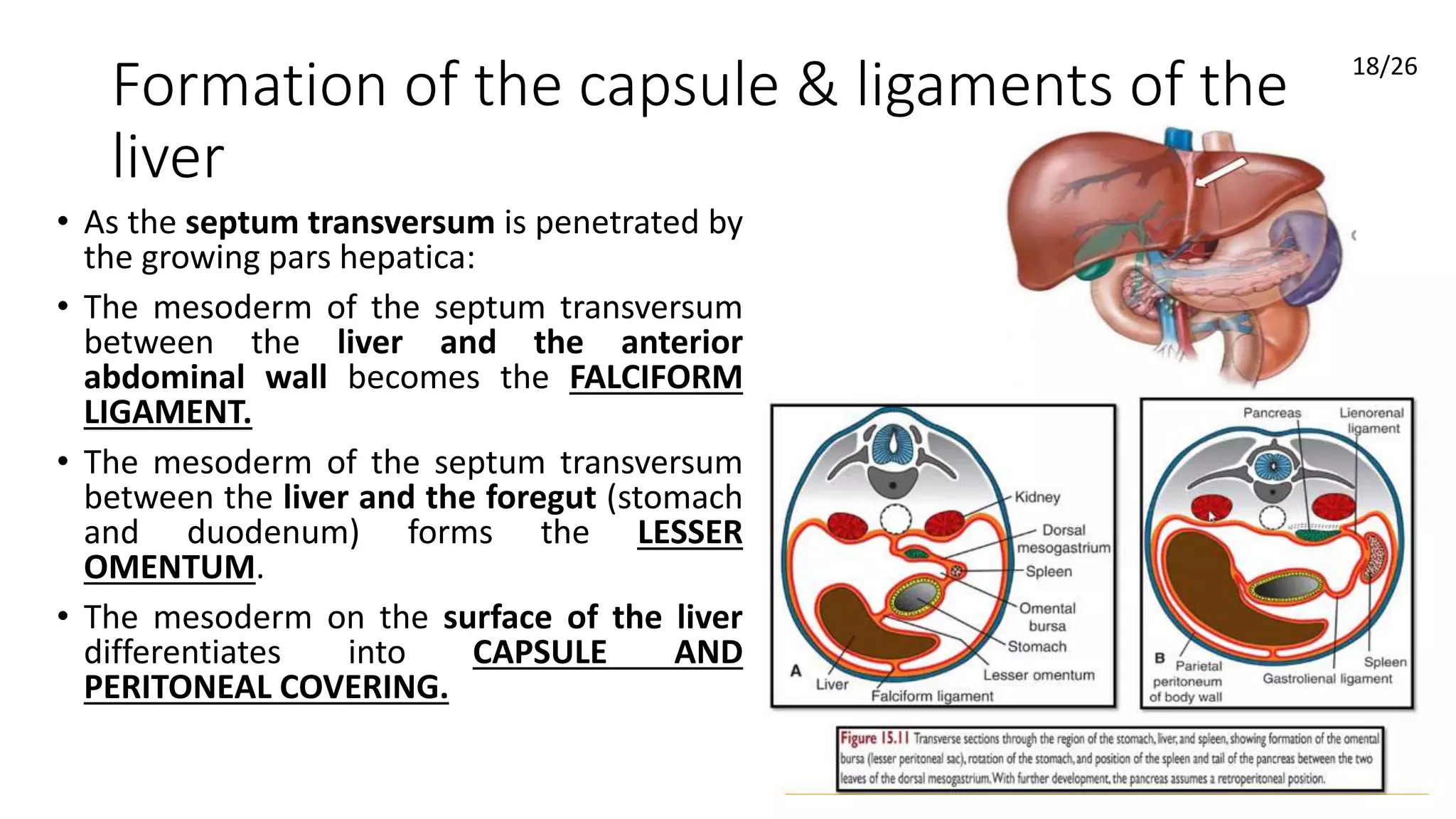








The liver develops from the endoderm of the foregut. During the 4th week, the hepatic diverticulum buds off from the foregut and divides into the pars hepatica and pars cystica. The pars hepatica gives rise to the liver parenchyma of hepatocytes and bile ducts. It expands between the layers of the septum transversum mesenchyme. The pars cystica develops into the gallbladder and cystic duct. By week 8, the basic structure of the liver and biliary tree is established.











































































































