Downloaded 65 times
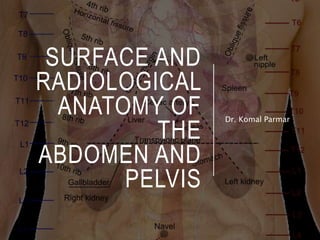
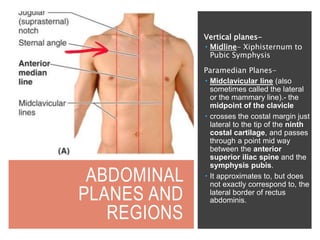
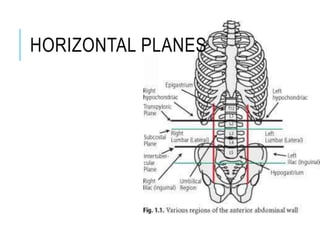

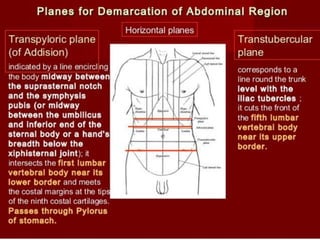
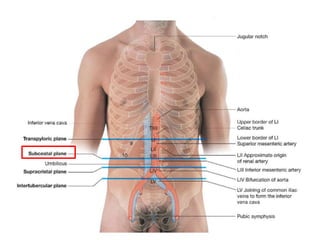
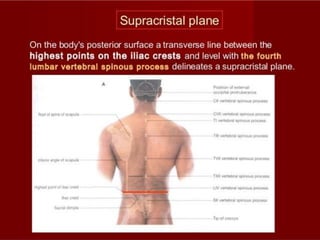
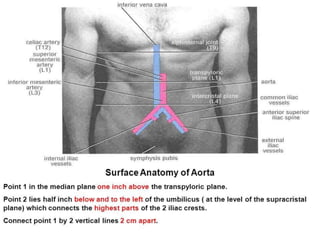
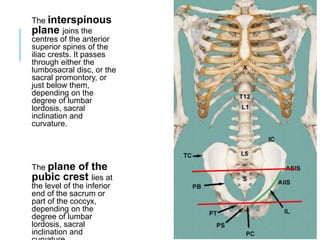

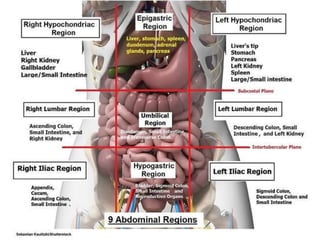
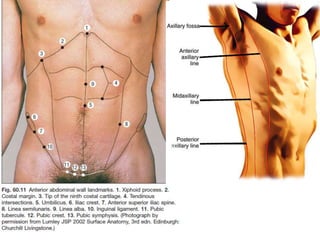
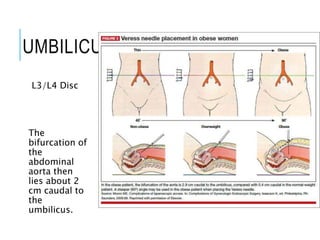
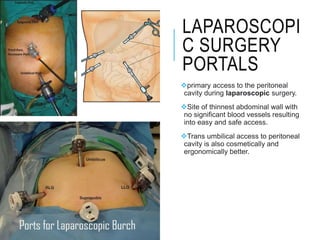
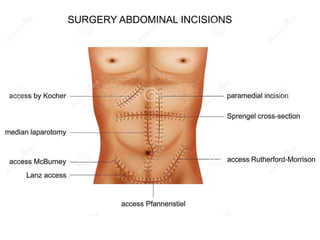



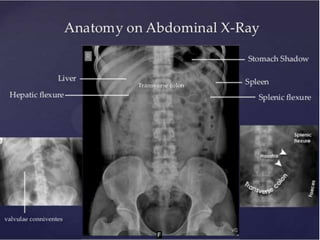

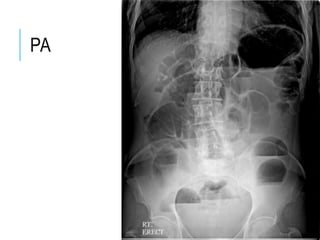
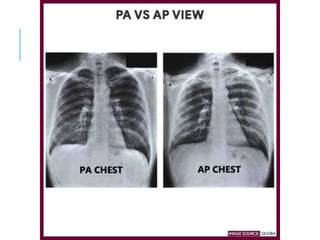


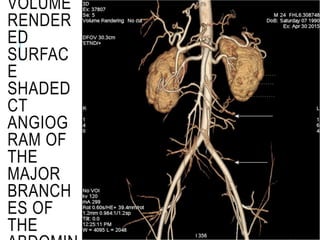
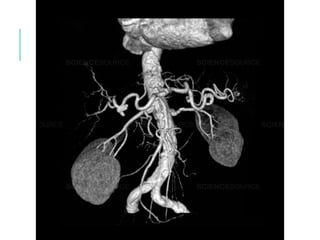
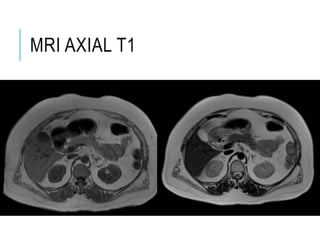

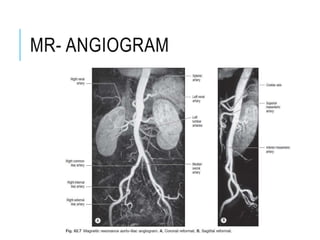











This document provides an overview of the surface and radiological anatomy of the abdomen and pelvis. It describes the abdominal planes and regions, including vertical, horizontal, and soft tissue landmarks. It also outlines various abdominal incisions and portals used in laparoscopic surgery. Finally, it reviews the radiological anatomy of intra-abdominal organs and various imaging modalities used to visualize the abdomen such as x-rays, CT, MRI, ultrasound, and endoscopy.