Downloaded 1,087 times


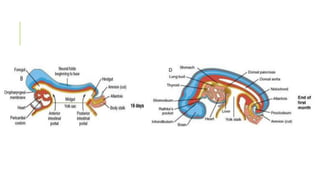



































The document summarizes the development of the gastrointestinal tract from the primitive gut tube through formation of the definitive foregut, midgut, and hindgut regions. Key points include: - The gut tube forms from endoderm lined yolk sac enveloped by mesoderm during folding. - The foregut gives rise to structures like the lungs, esophagus and stomach. The midgut forms the small intestine and parts of the large intestine. The hindgut forms the remaining large intestine. - Rotation and partitioning of the gut establishes the gut regions. Errors can cause clinical issues like esophageal atresia or intestinal malrotation.










































































