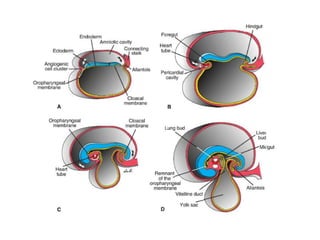
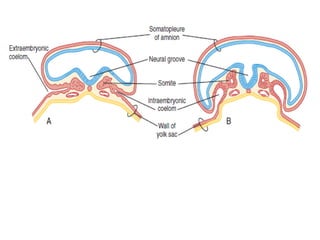
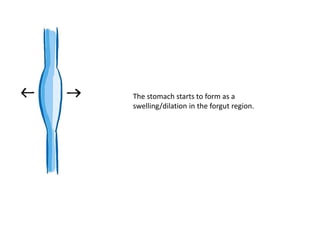
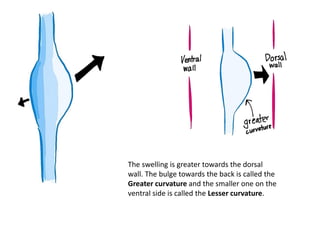
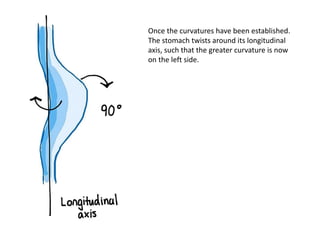
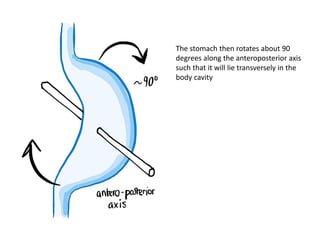
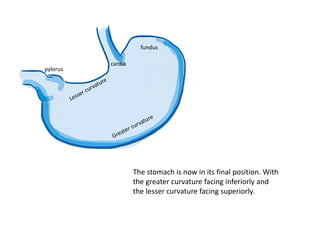
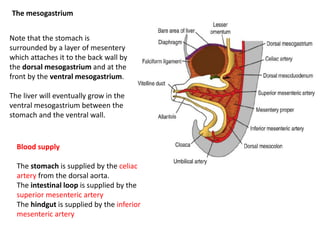
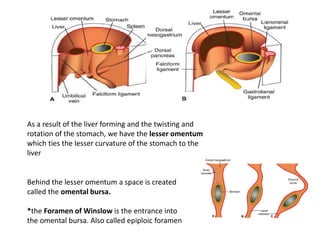
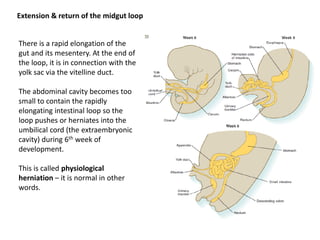
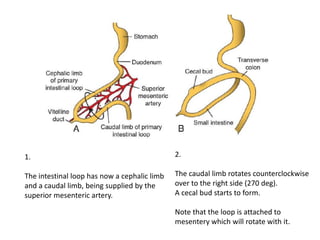
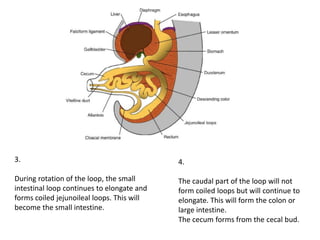
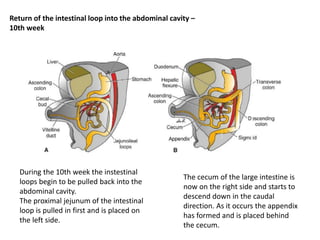
The document discusses the embryological development of the gastrointestinal (GI) tract, detailing the folding of the embryo post-gastrulation and the formation of the primitive gut tube which divides into foregut, midgut, and hindgut. It describes the stomach's formation, its rotation, and blood supply, along with the development of the small and large intestines, including the physiological herniation of the midgut loop. The document concludes with the separation of the hindgut and urogenital sinus, leading to the formation of distinct anatomical structures.