Downloaded 1,446 times
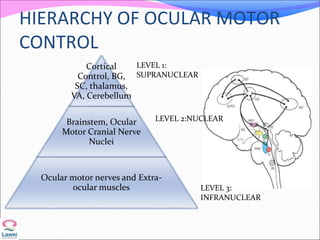
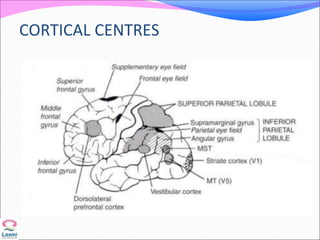
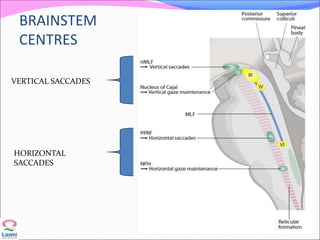
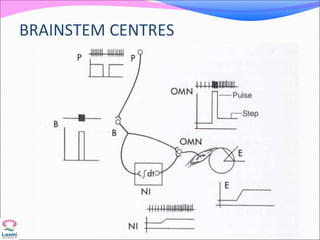
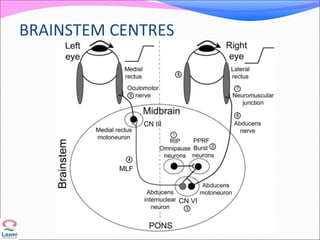

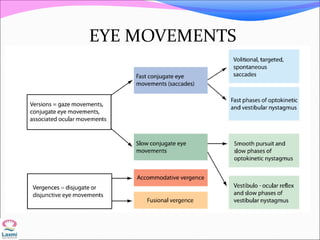
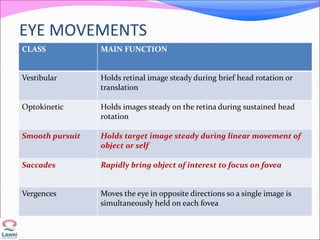
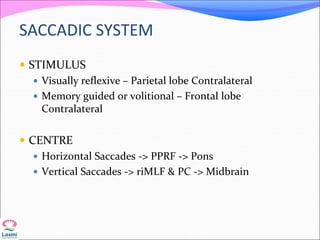
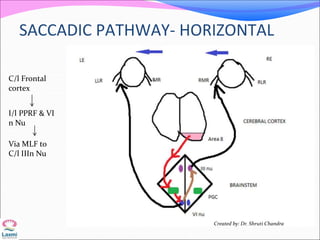
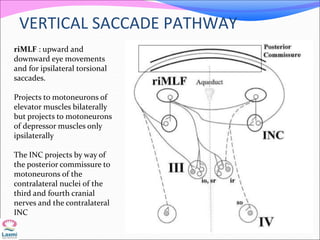
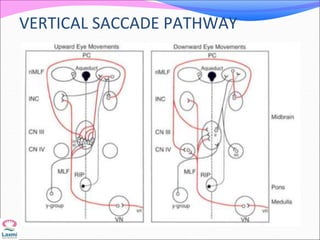
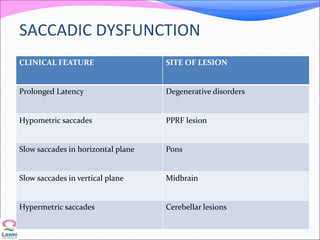
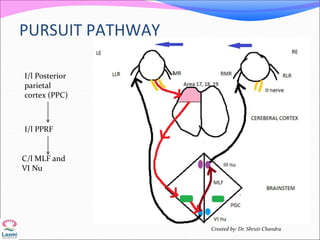
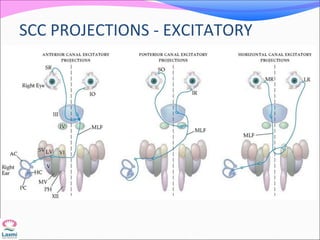
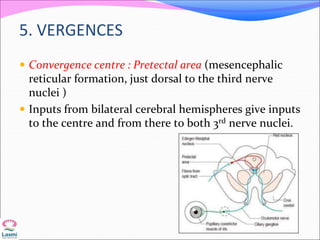


This document discusses supranuclear pathways and lesions that can affect eye movements. It begins with the fundamentals of extraocular movements and anatomy of cortical and brainstem centers that control eye movements. It then covers the basic types of eye movements like saccades, smooth pursuit, vestibular-ocular reflex, and vergence movements. It provides a step-wise approach to evaluating eye movement disorders and localizing lesions based on the type of eye movement affected. Supranuclear lesions can cause bilateral eye movement involvement, while specific brainstem lesions impact horizontal or vertical eye movements or specific eye movement types like saccades or vestibular-ocular reflex.