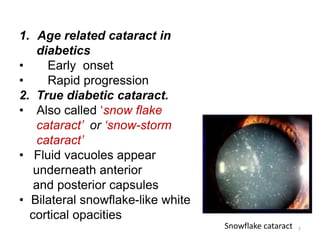
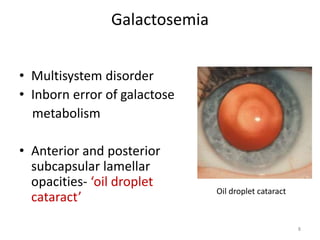
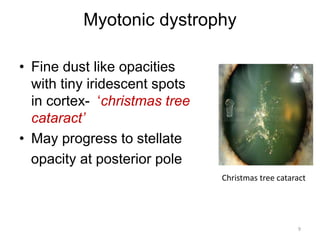
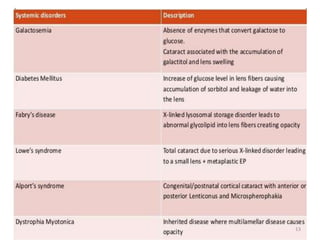
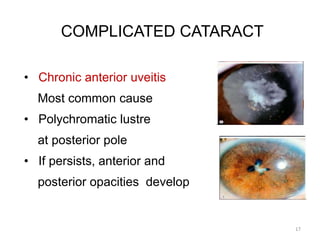
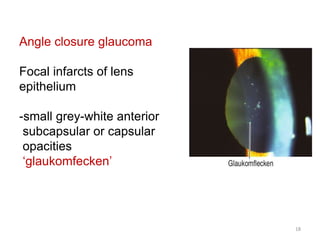
This document discusses metabolic and complicated cataracts. It defines cataract and provides a classification system that includes age-related, traumatic, metabolic, complicated, toxic, and radiation-induced cataracts. Metabolic cataracts are caused by endocrine disorders and biochemical abnormalities like diabetes and galactosemia. Complicated cataracts involve lens opacification secondary to other eye diseases such as uveitis or glaucoma. Specific types of metabolic and complicated cataracts are described along with their characteristic morphologies. Surgical management of cataracts involves evaluating patients, addressing underlying causes, and performing techniques like phacoemulsification or extracapsular extraction.