Downloaded 304 times






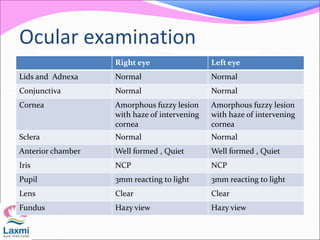





















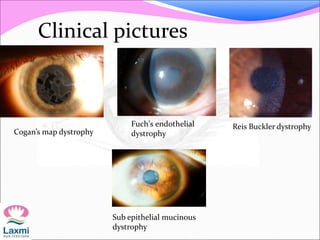


- Three cases of bilateral corneal opacities are presented - All cases show central corneal opacity without signs of inflammation or vascularization - This suggests a diagnosis of corneal dystrophy, which is a hereditary condition causing bilateral corneal opacity that is non-inflammatory in nature - Corneal dystrophy can be classified anatomically based on the layer of the cornea involved, or by the new IC3D classification system which integrates phenotype, pathology, and genetics























































































