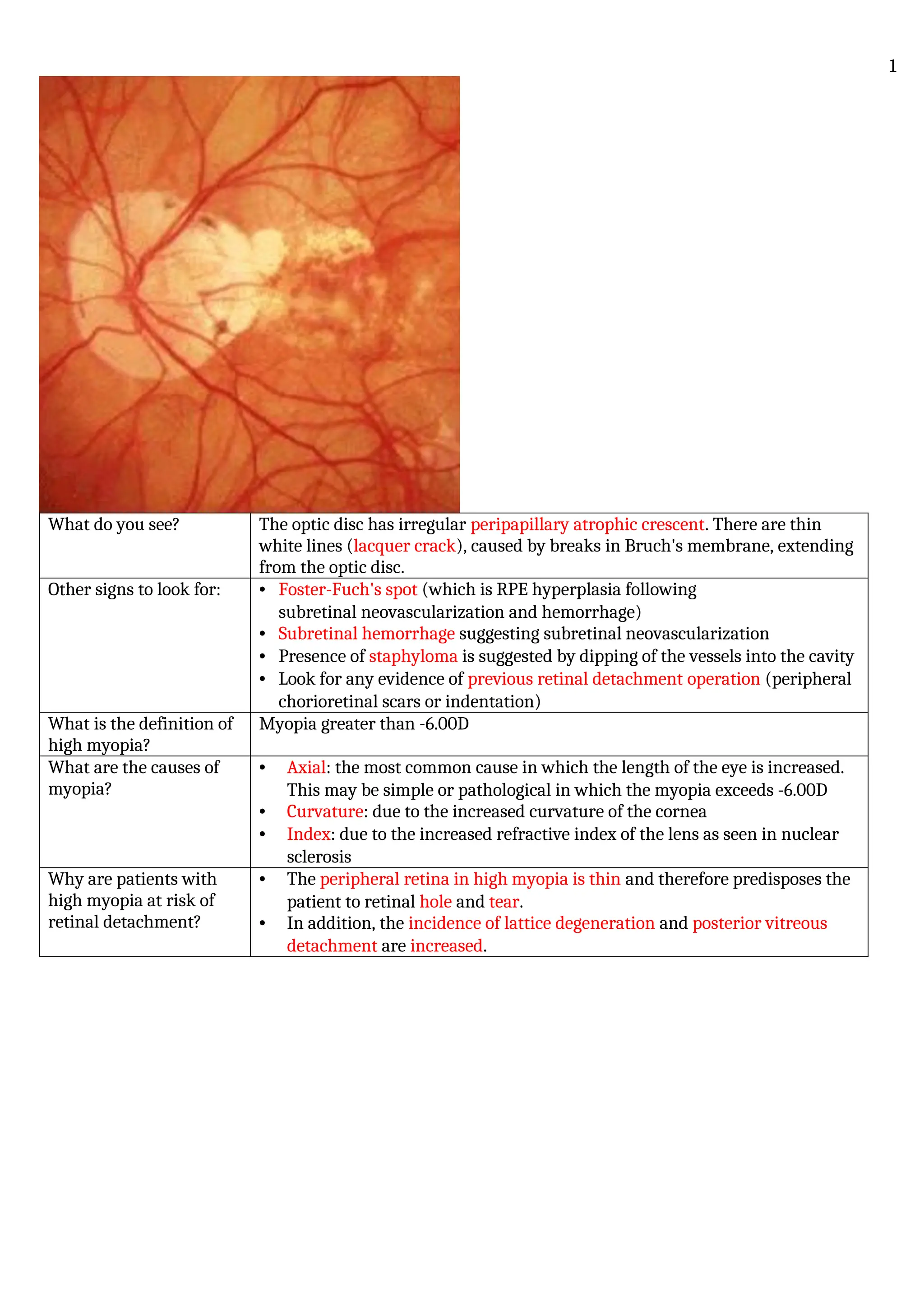
What do yousee? The optic disc has irregular peripapillary atrophic crescent. There are thin
white lines (lacquer crack), caused by breaks in Bruch's membrane, extending
from the optic disc.
Other signs to look for: • Foster-Fuch's spot (which is RPE hyperplasia following
subretinal neovascularization and hemorrhage)
• Subretinal hemorrhage suggesting subretinal neovascularization
• Presence of staphyloma is suggested by dipping of the vessels into the cavity
• Look for any evidence of previous retinal detachment operation (peripheral
chorioretinal scars or indentation)
What is the definition of
high myopia?
Myopia greater than -6.00D
What are the causes of
myopia?
• Axial: the most common cause in which the length of the eye is increased.
This may be simple or pathological in which the myopia exceeds -6.00D
• Curvature: due to the increased curvature of the cornea
• Index: due to the increased refractive index of the lens as seen in nuclear
sclerosis
Why are patients with
high myopia at risk of
retinal detachment?
• The peripheral retina in high myopia is thin and therefore predisposes the
patient to retinal hole and tear.
• In addition, the incidence of lattice degeneration and posterior vitreous
detachment are increased.
1
2.
What is thistechnique
called?
Regional eyelid block - Van Lint.
Infiltrate subcutaneously just outside the orbital margin with about 5ml of
lignocaine.
A common trigger of
neovascularization in
many eye diseases is
ischemia.
Can neovascularization
occur without significant
ischemia?
In wet age-related macular degeneration (AMD)
Where do new capillaries
grow from?
• In ischemic neovascularization from Branches of the retinal arteries
• In neovascularization in AMD from Choriocapillary layer
Is systemic drug
administration suitable
for the treatment of
retinal diseases?
NO. Because of poor drug permeability across the blood-retinal barrier:
- Complex tight junctions of retinal capillaries (inner)
- Complex junctions of retinal pigment epithelial cells (outer)
Can you break an acute
attack of angle closure
without medication?
By indenting the cornea.
• Push on the cornea through the patients closed eyelid. Press firmly and
hold for 10 seconds.
• Release and repeat ten times.
• Recheck the intraocular pressure. If the IOP seems unchanged repeat the
process once more.
• If the eye is noticeably softer, repeat with more gentle pressure until the
IOP seems normal.
• Apply force firmly and steadily.
• If the IOP falls quickly pain relief is almost immediate.
2
3.
What do yousee? Rubeosis Iridis
What is the significance
of AC examination?
The anterior chamber may contain cells, flare or even hyphema
What are the most
common causes you look
for in the posterior
segment?
• Central retinal vein occlusion
• Diabetic Retinopathy
What is 100-day
glaucoma?
Neovascular glaucoma secondary to ischemic CRVO
List some of the causes
for rubeotic glaucoma
• Most Common: CRVO and DR
• Other causes:
– Retinal artery occlusion
– Chronic RD
– Sickle cell retinopathy
– Radiation retinopathy
– Carotid artery occlusive disease
– Chronic uveitis
3
4.
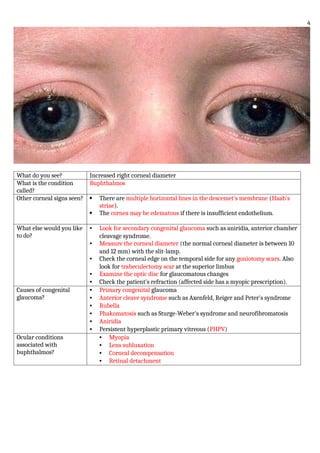
What do yousee? Increased right corneal diameter
What is the condition
called?
Buphthalmos
Other corneal signs seen? There are multiple horizontal lines in the descemet's membrane (Haab's
striae).
The cornea may be edematous if there is insufficient endothelium.
What else would you like
to do?
• Look for secondary congenital glaucoma such as aniridia, anterior chamber
cleavage syndrome.
• Measure the corneal diameter (the normal corneal diameter is between 10
and 12 mm) with the slit-lamp.
• Check the corneal edge on the temporal side for any goniotomy scars. Also
look for trabeculectomy scar at the superior limbus
• Examine the optic disc for glaucomatous changes
• Check the patient's refraction (affected side has a myopic prescription).
Causes of congenital
glaucoma?
• Primary congenital glaucoma
• Anterior cleave syndrome such as Axenfeld, Reiger and Peter's syndrome
• Rubella
• Phakomatosis such as Sturge-Weber's syndrome and neurofibromatosis
• Aniridia
• Persistent hyperplastic primary vitreous (PHPV)
Ocular conditions
associated with
buphthalmos?
• Myopia
• Lens subluxation
• Corneal decompensation
• Retinal detachment
4
5.
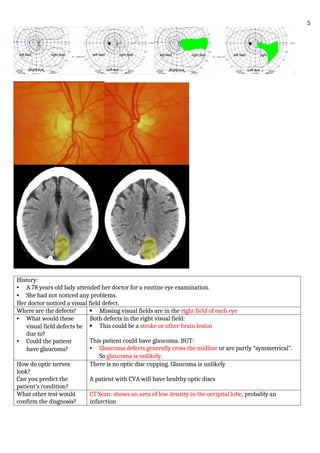
History:
• A 78years old lady attended her doctor for a routine eye examination.
• She had not noticed any problems.
Her doctor noticed a visual field defect.
Where are the defects? Missing visual fields are in the right field of each eye
• What would these
visual field defects be
due to?
• Could the patient
have glaucoma?
Both defects in the right visual field:
This could be a stroke or other brain lesion
This patient could have glaucoma. BUT:
• Glaucoma defects generally cross the midline or are partly “symmetrical”.
So glaucoma is unlikely.
How do optic nerves
look?
Can you predict the
patient’s condition?
There is no optic disc cupping. Glaucoma is unlikely
A patient with CVA will have healthy optic discs
What other test would
confirm the diagnosis?
CT Scan: shows an area of low density in the occipital lobe, probably an
infarction
5
6.
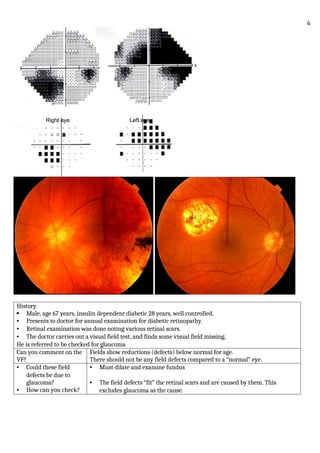
History
Male, age67 years, insulin dependent diabetic 28 years, well controlled.
• Presents to doctor for annual examination for diabetic retinopathy.
• Retinal examination was done noting various retinal scars.
• The doctor carries out a visual field test, and finds some visual field missing.
He is referred to be checked for glaucoma
Can you comment on the
VF?
Fields show reductions (defects) below normal for age.
There should not be any field defects compared to a “normal” eye.
• Could these field
defects be due to
glaucoma?
• How can you check?
• Must dilate and examine fundus
• The field defects “fit” the retinal scars and are caused by them. This
excludes glaucoma as the cause.
6
7.
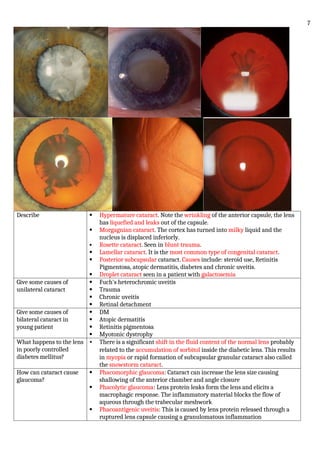
Describe Hypermaturecataract. Note the wrinkling of the anterior capsule, the lens
has liquefied and leaks out of the capsule.
Morgagnian cataract. The cortex has turned into milky liquid and the
nucleus is displaced inferiorly.
Rosette cataract. Seen in blunt trauma.
Lamellar cataract. It is the most common type of congenital cataract.
Posterior subcapsular cataract. Causes include: steroid use, Retinitis
Pigmentosa, atopic dermatitis, diabetes and chronic uveitis.
Droplet cataract seen in a patient with galactosemia
Give some causes of
unilateral cataract
Fuch's heterochromic uveitis
Trauma
Chronic uveitis
Retinal detachment
Give some causes of
bilateral cataract in
young patient
DM
Atopic dermatitis
Retinitis pigmentosa
Myotonic dystrophy
What happens to the lens
in poorly controlled
diabetes mellitus?
• There is a significant shift in the fluid content of the normal lens probably
related to the accumulation of sorbitol inside the diabetic lens. This results
in myopia or rapid formation of subcapsular granular cataract also called
the snowstorm cataract.
How can cataract cause
glaucoma?
Phacomorphic glaucoma: Cataract can increase the lens size causing
shallowing of the anterior chamber and angle closure
Phacolytic glaucoma: Lens protein leaks form the lens and elicits a
macrophagic response. The inflammatory material blocks the flow of
aqueous through the trabecular meshwork
Phacoantigenic uveitis: This is caused by lens protein released through a
ruptured lens capsule causing a granulomatous inflammation
7
8.
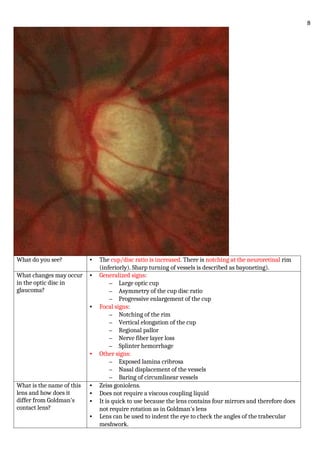
What do yousee? • The cup/disc ratio is increased. There is notching at the neuroretinal rim
(inferiorly). Sharp turning of vessels is described as bayoneting).
What changes may occur
in the optic disc in
glaucoma?
• Generalized signs:
– Large optic cup
– Asymmetry of the cup disc ratio
– Progressive enlargement of the cup
• Focal signs:
– Notching of the rim
– Vertical elongation of the cup
– Regional pallor
– Nerve fiber layer loss
– Splinter hemorrhage
• Other signs:
– Exposed lamina cribrosa
– Nasal displacement of the vessels
– Baring of circumlinear vessels
What is the name of this
lens and how does it
differ from Goldman's
contact lens?
• Zeiss goniolens.
• Does not require a viscous coupling liquid
• It is quick to use because the lens contains four mirrors and therefore does
not require rotation as in Goldman's lens
• Lens can be used to indent the eye to check the angles of the trabecular
meshwork.
8
9.
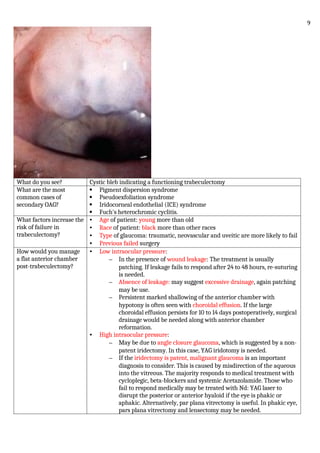
What do yousee? Cystic bleb indicating a functioning trabeculectomy
What are the most
common cases of
secondary OAG?
Pigment dispersion syndrome
Pseudoexfoliation syndrome
Iridocorneal endothelial (ICE) syndrome
Fuch's heterochromic cyclitis.
What factors increase the
risk of failure in
trabeculectomy?
• Age of patient: young more than old
• Race of patient: black more than other races
• Type of glaucoma: traumatic, neovascular and uveitic are more likely to fail
• Previous failed surgery
How would you manage
a flat anterior chamber
post-trabeculectomy?
• Low intraocular pressure:
– In the presence of wound leakage: The treatment is usually
patching. If leakage fails to respond after 24 to 48 hours, re-suturing
is needed.
– Absence of leakage: may suggest excessive drainage, again patching
may be use.
– Persistent marked shallowing of the anterior chamber with
hypotony is often seen with choroidal effusion. If the large
choroidal effusion persists for 10 to 14 days postoperatively, surgical
drainage would be needed along with anterior chamber
reformation.
• High intraocular pressure:
– May be due to angle closure glaucoma, which is suggested by a non-
patent iridectomy. In this case, YAG iridotomy is needed.
– If the iridectomy is patent, malignant glaucoma is an important
diagnosis to consider. This is caused by misdirection of the aqueous
into the vitreous. The majority responds to medical treatment with
cycloplegic, beta-blockers and systemic Acetazolamide. Those who
fail to respond medically may be treated with Nd: YAG laser to
disrupt the posterior or anterior hyaloid if the eye is phakic or
aphakic. Alternatively, par plana vitrectomy is useful. In phakic eye,
pars plana vitrectomy and lensectomy may be needed.
9
10.
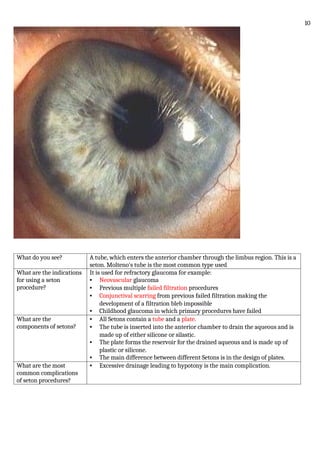
What do yousee? A tube, which enters the anterior chamber through the limbus region. This is a
seton. Molteno's tube is the most common type used
What are the indications
for using a seton
procedure?
It is used for refractory glaucoma for example:
• Neovascular glaucoma
• Previous multiple failed filtration procedures
• Conjunctival scarring from previous failed filtration making the
development of a filtration bleb impossible
• Childhood glaucoma in which primary procedures have failed
What are the
components of setons?
• All Setons contain a tube and a plate.
• The tube is inserted into the anterior chamber to drain the aqueous and is
made up of either silicone or silastic.
• The plate forms the reservoir for the drained aqueous and is made up of
plastic or silicone.
• The main difference between different Setons is in the design of plates.
What are the most
common complications
of seton procedures?
• Excessive drainage leading to hypotony is the main complication.
10
11.
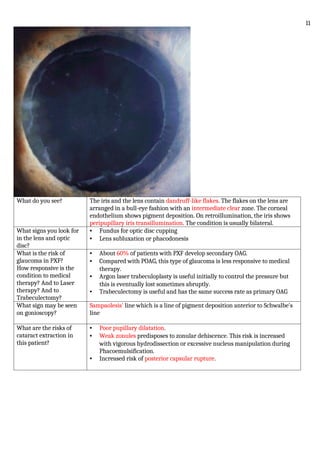
What do yousee? The iris and the lens contain dandruff-like flakes. The flakes on the lens are
arranged in a bull-eye fashion with an intermediate clear zone. The corneal
endothelium shows pigment deposition. On retroillumination, the iris shows
peripupillary iris transillumination. The condition is usually bilateral.
What signs you look for
in the lens and optic
disc?
• Fundus for optic disc cupping
• Lens subluxation or phacodonesis
What is the risk of
glaucoma in PXF?
How responsive is the
condition to medical
therapy? And to Laser
therapy? And to
Trabeculectomy?
• About 60% of patients with PXF develop secondary OAG.
• Compared with POAG, this type of glaucoma is less responsive to medical
therapy.
• Argon laser trabeculoplasty is useful initially to control the pressure but
this is eventually lost sometimes abruptly.
• Trabeculectomy is useful and has the same success rate as primary OAG
What sign may be seen
on gonioscopy?
Sampaolesis' line which is a line of pigment deposition anterior to Schwalbe's
line
What are the risks of
cataract extraction in
this patient?
• Poor pupillary dilatation.
• Weak zonules predisposes to zonular dehiscence. This risk is increased
with vigorous hydrodissection or excessive nucleus manipulation during
Phacoemulsification.
• Increased risk of posterior capsular rupture.
11
12.
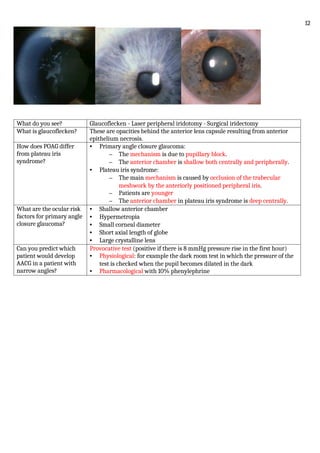
What do yousee? Glaucoflecken - Laser peripheral iridotomy - Surgical iridectomy
What is glaucoflecken? These are opacities behind the anterior lens capsule resulting from anterior
epithelium necrosis.
How does POAG differ
from plateau iris
syndrome?
• Primary angle closure glaucoma:
– The mechanism is due to pupillary block.
– The anterior chamber is shallow both centrally and peripherally.
• Plateau iris syndrome:
– The main mechanism is caused by occlusion of the trabecular
meshwork by the anteriorly positioned peripheral iris.
– Patients are younger
– The anterior chamber in plateau iris syndrome is deep centrally.
What are the ocular risk
factors for primary angle
closure glaucoma?
• Shallow anterior chamber
• Hypermetropia
• Small corneal diameter
• Short axial length of globe
• Large crystalline lens
Can you predict which
patient would develop
AACG in a patient with
narrow angles?
Provocative test (positive if there is 8 mmHg pressure rise in the first hour)
• Physiological: for example the dark room test in which the pressure of the
test is checked when the pupil becomes dilated in the dark
• Pharmacological with 10% phenylephrine
12
13.
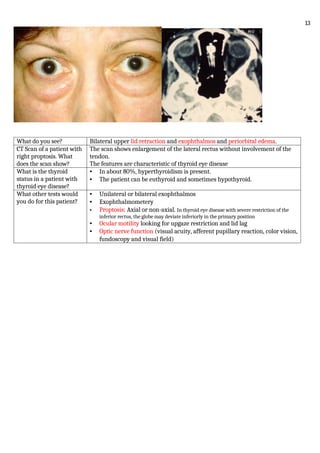
What do yousee? Bilateral upper lid retraction and exophthalmos and periorbital edema.
CT Scan of a patient with
right proptosis. What
does the scan show?
The scan shows enlargement of the lateral rectus without involvement of the
tendon.
The features are characteristic of thyroid eye disease
What is the thyroid
status in a patient with
thyroid eye disease?
• In about 80%, hyperthyroidism is present.
• The patient can be euthyroid and sometimes hypothyroid.
What other tests would
you do for this patient?
• Unilateral or bilateral exophthalmos
• Exophthalmometery
• Proptosis: Axial or non-axial. In thyroid eye disease with severe restriction of the
inferior rectus, the globe may deviate inferiorly in the primary position
• Ocular motility looking for upgaze restriction and lid lag
• Optic nerve function (visual acuity, afferent pupillary reaction, color vision,
fundoscopy and visual field)
13
14.
What do yousee?
What procedure is used
to see it?
What examination clues
are used to determine the
underlying cause?
Iris transillumination
• Retro-illumination
• The distribution of the transillumination
• Common types:
– Peripapillary: Pseudoexfoliation syndrome
– Mid-periphery: Pigment dispersion syndrome
– Diffuse: albinism, previous acute angle closure glaucoma, Fuchs'
heterochromic cyclitis, senile iris atrophy, post-cataract extraction
– Sectoral:
– Herpes zoster iritis
– Iris prolapse during Phacoemulsification
14
15.
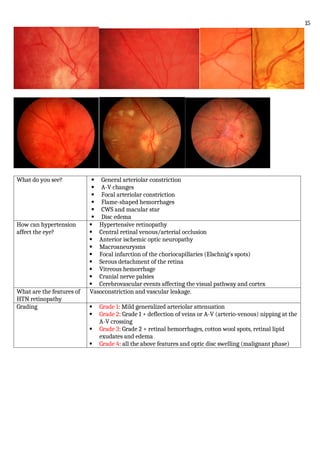
What do yousee? General arteriolar constriction
A-V changes
Focal arteriolar constriction
Flame-shaped hemorrhages
CWS and macular star
Disc edema
How can hypertension
affect the eye?
Hypertensive retinopathy
Central retinal venous/arterial occlusion
Anterior ischemic optic neuropathy
Macroaneurysms
Focal infarction of the choriocapillaries (Elschnig's spots)
Serous detachment of the retina
Vitreous hemorrhage
Cranial nerve palsies
Cerebrovascular events affecting the visual pathway and cortex
What are the features of
HTN retinopathy
Vasoconstriction and vascular leakage.
Grading Grade 1: Mild generalized arteriolar attenuation
Grade 2: Grade 1 + deflection of veins or A-V (arterio-venous) nipping at the
A-V crossing
Grade 3: Grade 2 + retinal hemorrhages, cotton wool spots, retinal lipid
exudates and edema
Grade 4: all the above features and optic disc swelling (malignant phase)
15
16.
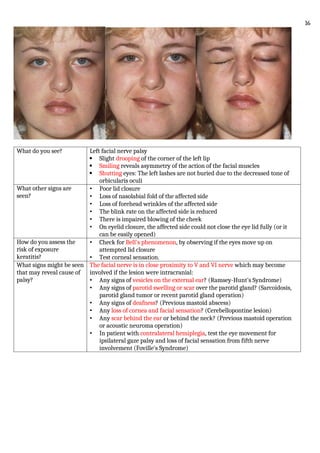
What do yousee? Left facial nerve palsy
Slight drooping of the corner of the left lip
Smiling reveals asymmetry of the action of the facial muscles
Shutting eyes: The left lashes are not buried due to the decreased tone of
orbicularis oculi
What other signs are
seen?
• Poor lid closure
• Loss of nasolabial fold of the affected side
• Loss of forehead wrinkles of the affected side
• The blink rate on the affected side is reduced
• There is impaired blowing of the cheek
• On eyelid closure, the affected side could not close the eye lid fully (or it
can be easily opened)
How do you assess the
risk of exposure
keratitis?
• Check for Bell's phenomenon, by observing if the eyes move up on
attempted lid closure
• Test corneal sensation.
What signs might be seen
that may reveal cause of
palsy?
The facial nerve is in close proximity to V and VI nerve which may become
involved if the lesion were intracranial:
• Any signs of vesicles on the external ear? (Ramsey-Hunt's Syndrome)
• Any signs of parotid swelling or scar over the parotid gland? (Sarcoidosis,
parotid gland tumor or recent parotid gland operation)
• Any signs of deafness? (Previous mastoid abscess)
• Any loss of cornea and facial sensation? (Cerebellopontine lesion)
• Any scar behind the ear or behind the neck? (Previous mastoid operation
or acoustic neuroma operation)
• In patient with contralateral hemiplegia, test the eye movement for
ipsilateral gaze palsy and loss of facial sensation from fifth nerve
involvement (Foville's Syndrome)
16
17.
This Patient wasasked to
keep a sustained upgaze.
What do you see?
Right ptosis of the right lid due to fatigue
Signs in myasthenia • Partial ptosis.
• Pupils are equal in size.
• Limitation of ocular movement in any combination.
The vertical muscles tend to be affected most. The limitation is variable
and does not appear to correspond to any nerve palsy.
• On sustained upgaze, the affected upper lid shows increased ptosis.
• Cogan's lid twitch sign: Let the patient rapidly refixate their eye from
downgaze to the primary position, the sign is positive if there is
overshooting of the upper lid before settling down to the ptotic position
Other signs of myasthenia gravis: thoracic scar from thymomectomy
How would you perform
ice pack test?
• Ice is applied over the ptotic eye for two minutes.
• In a patient with myasthenia gravis, the ptosis improves.
17
18.
8-year-old girl presenteda 5-day history of swollen right eye, which
was unresponsive to oral Augmentin prescribed by her GP
CT Scan: Right proptosis with opacification
of the right Ethmoidal sinus
Compare preseptal to orbital
cellulitis.
Signs, causing organisms and
management
Inflammation and infection
confined to lids and periorbita
anterior to septum
Infection posterior to orbital septum &
frequently poly-microbial
80% of patients < 10 years and most
patients < 5 years
Usually 2ry to trauma or skin
infection in children and adults
90% due to extension of acute or chronic
bacterial sinusitis; remainder are post
traumatic or surgery or 2ry to extension
from other orbital or periorbital infection,
or endogenous with hematogenous spread
Most common organisms are Staph
aureus, Staph epidermidis, Strept
species, and anaerobes
Most common organisms are Strept
pneumonia, staph aureus, strept pyogenes,
H influenza
Tender, red, periorbita and lid
swelling. Patient is well, no fever
Rapid onset of sever malaise & fever
Swollen lids, red, warm and tender
Visual acuity, Pupils, EOM
movement are all intact; No
proptosis
Proptosis (lateral & down), Restriction of
EOM’s, Pain on globe movement
Teenagers and adults can be closely
followed as outpatients with PO
antibiotics
Do CT Scan of orbit and sinuses to confirm
sinus disease, rule out mass or orbital
foreign body, rule out orbital or sub-
periosteal abscess
Children under 5 years may have
bacteremia. It is a more severe
disease, need IV 3rd generation
cephalosporin antibiotics
• Admit to hospital
• Do Blood culture & start broad
spectrum IV antibiotics to cover gram
+ve cocci, H. influenza, anaerobes
• Children: ampicillin + cloxacillin
• Adults: Typically nafcillin and 3rd
generation cephalosporin and
metronidazole
Surgical drainage of abscess may be
necessary; do not violate septum
and cause orbital cellulitis
Monitor O. N. functions every 4 hours: VA,
Pupillary reactions, color vision, light
brightness; also monitor temperature,
proptosis and EOM restriction
Progress of infection or no
improvement means
Abscess: repeat CT as needed and drain
abscess and sinus as needed
Decreased VA, RAPD,
prolonged high IOP means
Orbital apex syndrome or cavernous sinus
thrombosis
18
19.
A 24-year-old manpresents after a fight. He was struck in the face multiple times. He presents with severe
pain on the left side of the face, subcutaneous emphysema of the left eyelid, and numbness over the left
cheek. The patient has vertical diplopia.
An orbital CT is
performed revealing
fractures of what
structures?
A. Lamina papyracea
B. Maxillary sinus
C. Nasal bone
D. Orbital floor
E. Zygomatic arch
What happens to soft
tissue in such a trauma
May herniate into the maxillary sinus, leading to entrapment and vertical
diplopia
Management Includes analgesics, ice, and oculoplastic consultation
19
20.
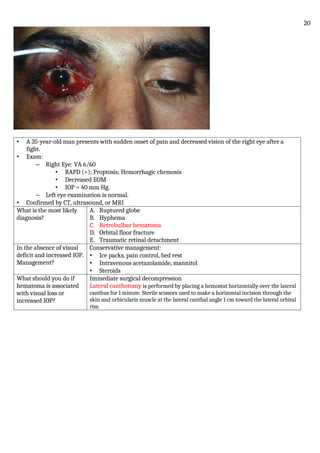
• A 35-year-oldman presents with sudden onset of pain and decreased vision of the right eye after a
fight.
• Exam:
– Right Eye: VA 6/60
• RAPD (+); Proptosis; Hemorrhagic chemosis
• Decreased EOM
• IOP = 40 mm Hg.
– Left eye examination is normal.
• Confirmed by CT, ultrasound, or MRI
What is the most likely
diagnosis?
A. Ruptured globe
B. Hyphema
C. Retrobulbar hematoma
D. Orbital floor fracture
E. Traumatic retinal detachment
In the absence of visual
deficit and increased IOP.
Management?
Conservative management:
• Ice packs, pain control, bed rest
• Intravenous acetazolamide, mannitol
• Steroids
What should you do if
hematoma is associated
with visual loss or
increased IOP?
Immediate surgical decompression
Lateral canthotomy is performed by placing a hemostat horizontally over the lateral
canthus for 1 minute. Sterile scissors used to make a horizontal incision through the
skin and orbicularis muscle at the lateral canthal angle 1 cm toward the lateral orbital
rim
20
21.
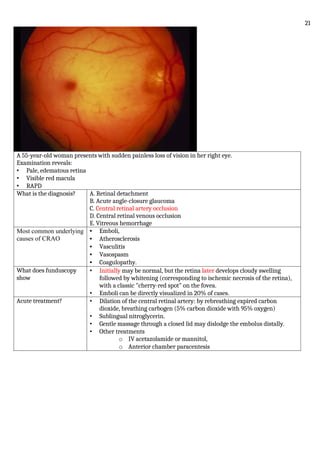
A 55-year-old womanpresents with sudden painless loss of vision in her right eye.
Examination reveals:
• Pale, edematous retina
• Visible red macula
• RAPD
What is the diagnosis? A. Retinal detachment
B. Acute angle-closure glaucoma
C. Central retinal artery occlusion
D. Central retinal venous occlusion
E. Vitreous hemorrhage
Most common underlying
causes of CRAO
• Emboli,
• Atherosclerosis
• Vasculitis
• Vasospasm
• Coagulopathy.
What does funduscopy
show
• Initially may be normal, but the retina later develops cloudy swelling
followed by whitening (corresponding to ischemic necrosis of the retina),
with a classic "cherry-red spot" on the fovea.
• Emboli can be directly visualized in 20% of cases.
Acute treatment? • Dilation of the central retinal artery: by rebreathing expired carbon
dioxide, breathing carbogen (5% carbon dioxide with 95% oxygen)
• Sublingual nitroglycerin.
• Gentle massage through a closed lid may dislodge the embolus distally.
• Other treatments
o IV acetazolamide or mannitol,
o Anterior chamber paracentesis
21
22.
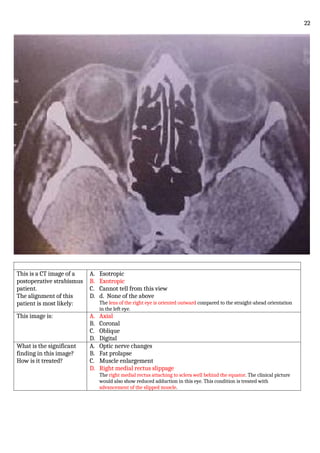
This is aCT image of a
postoperative strabismus
patient.
The alignment of this
patient is most likely:
A. Esotropic
B. Exotropic
C. Cannot tell from this view
D. d. None of the above
The lens of the right eye is oriented outward compared to the straight-ahead orientation
in the left eye.
This image is: A. Axial
B. Coronal
C. Oblique
D. Digital
What is the significant
finding in this image?
How is it treated?
A. Optic nerve changes
B. Fat prolapse
C. Muscle enlargement
D. Right medial rectus slippage
The right medial rectus attaching to sclera well behind the equator. The clinical picture
would also show reduced adduction in this eye. This condition is treated with
advancement of the slipped muscle.
22









































![Acute visual loss [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/acutevisuallosscompatibilitymode-220808143729-7342aaf9-thumbnail.jpg?width=640&height=640&fit=bounds)
![AQEOUS_HUMOUR_PHYSIOLOGY_AND_GLAUCOMA3_(1)[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aqeoushumourphysiologyandglaucoma311-250407162804-3ddea82a-thumbnail.jpg?width=640&height=640&fit=bounds)






































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












