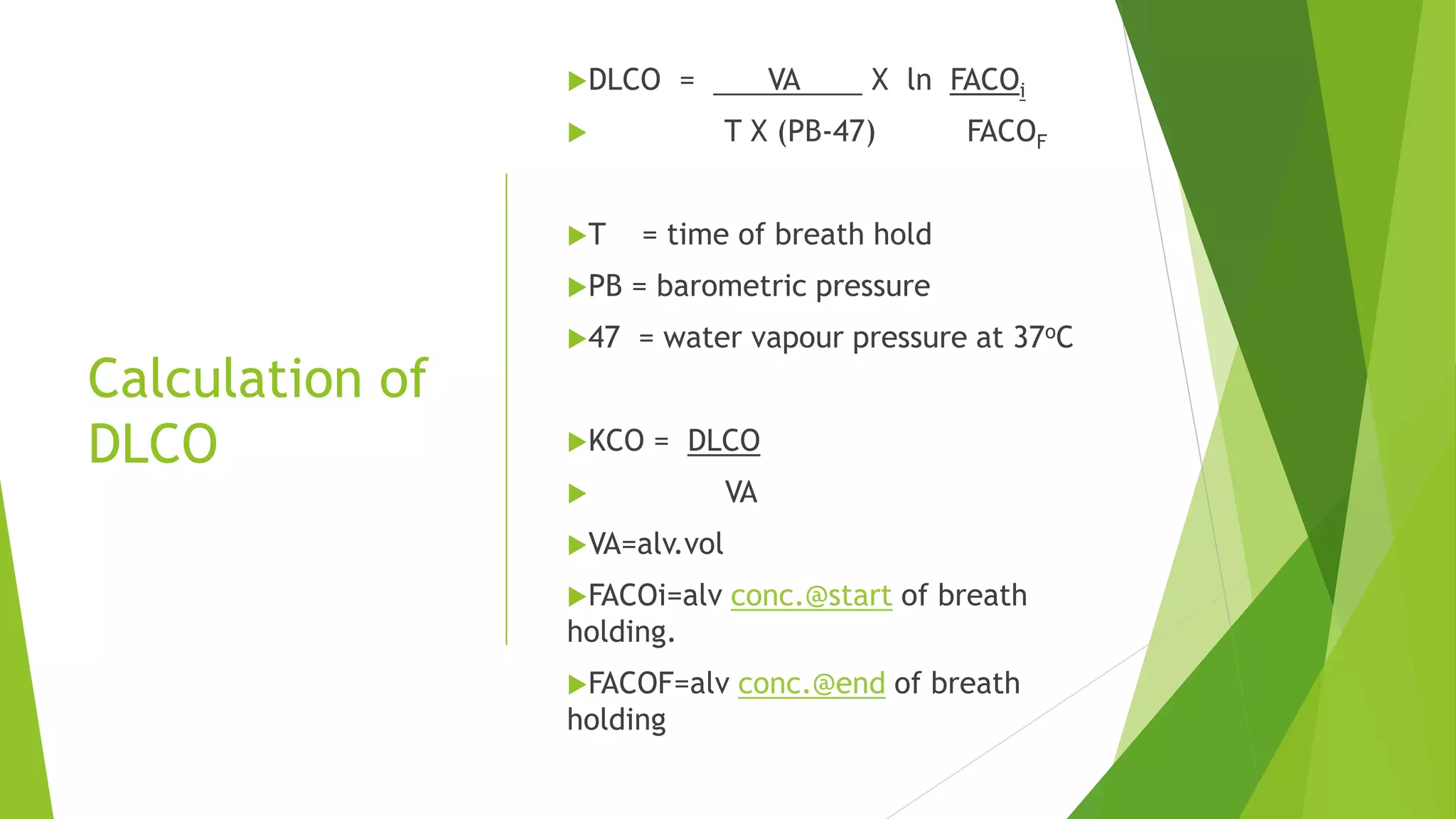
1. The document discusses DLCO (diffusing capacity of the lungs for carbon monoxide), which measures the efficiency of the lungs in transporting oxygen across the alveolar capillary membrane.
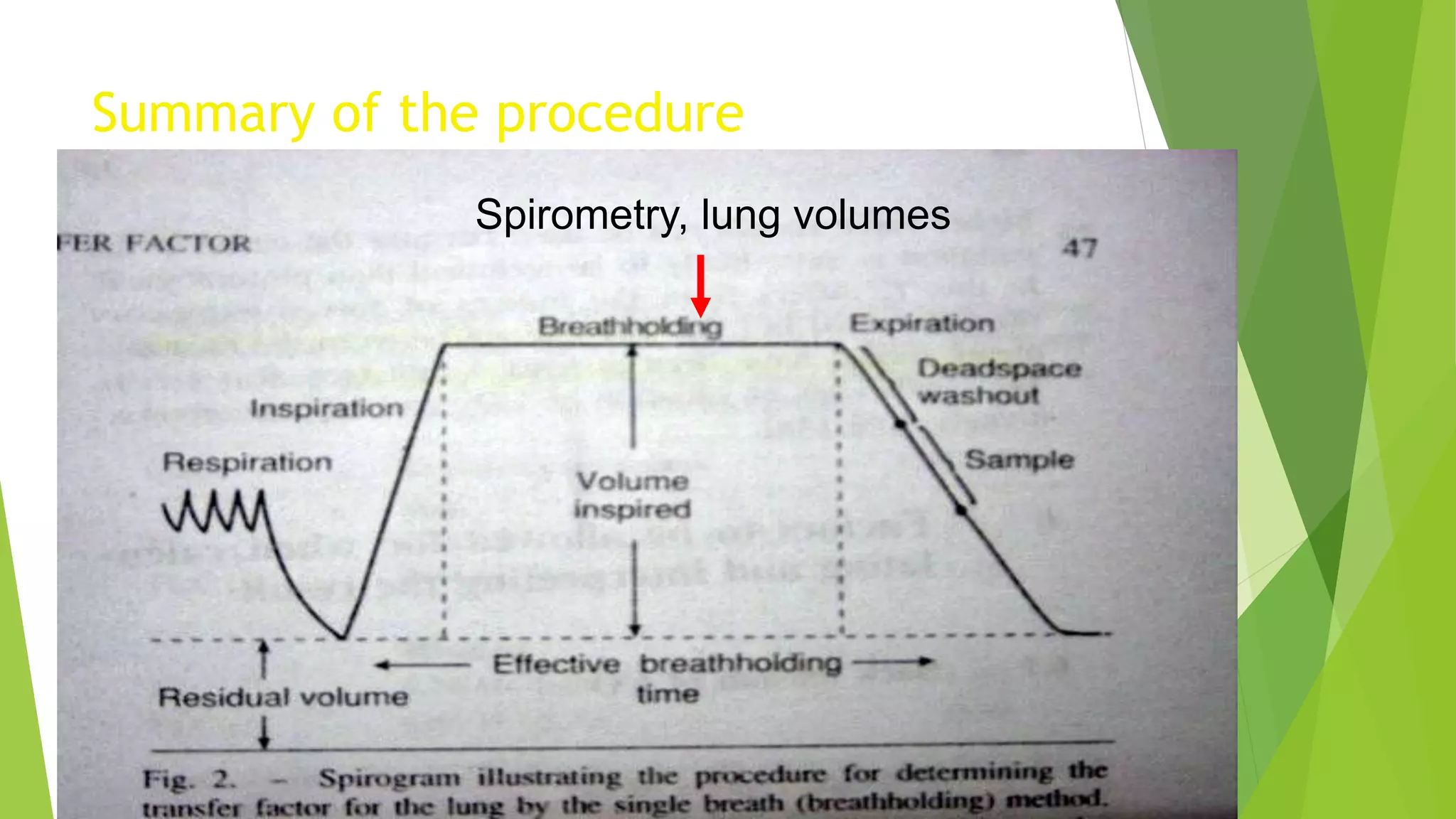
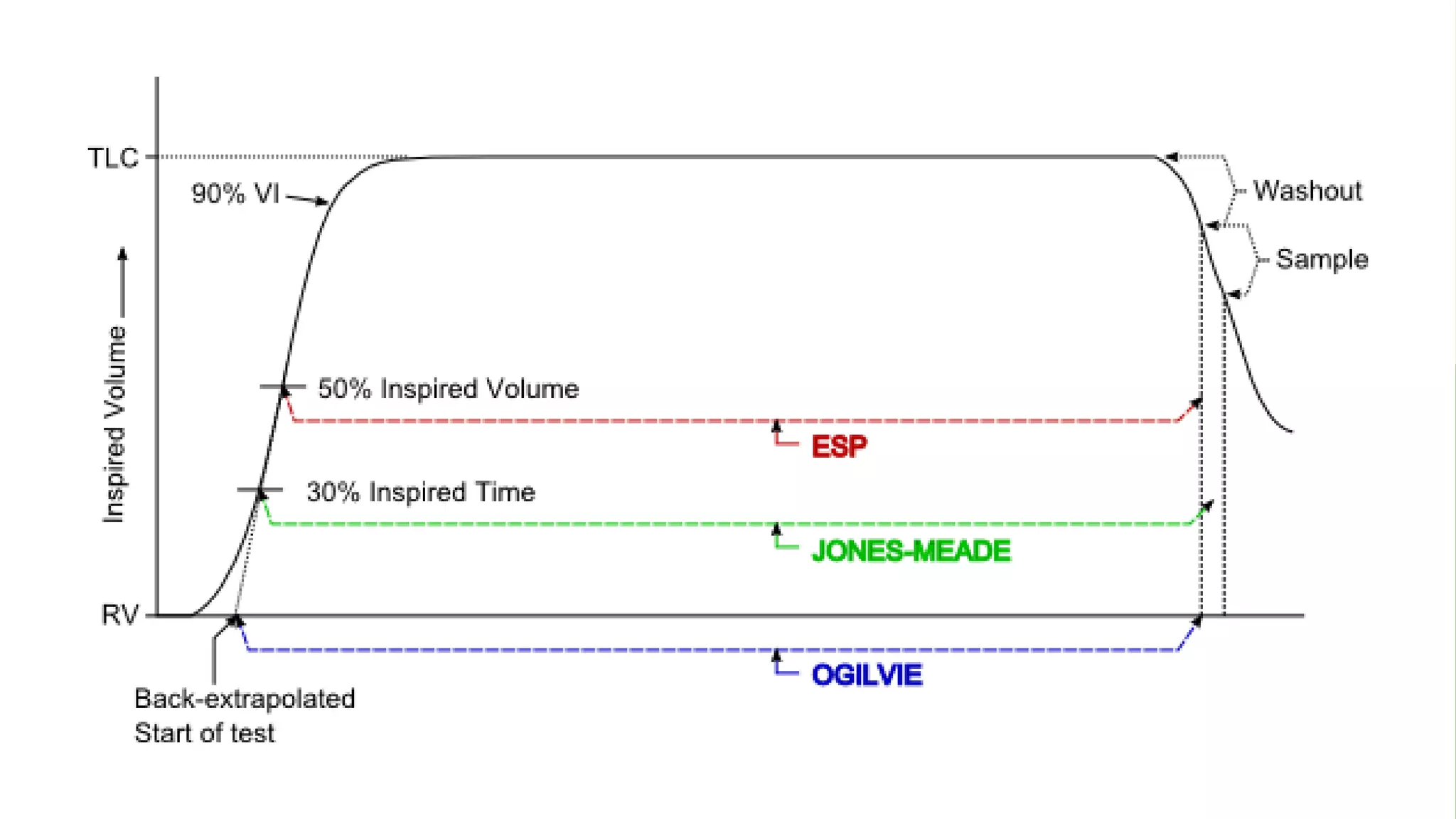
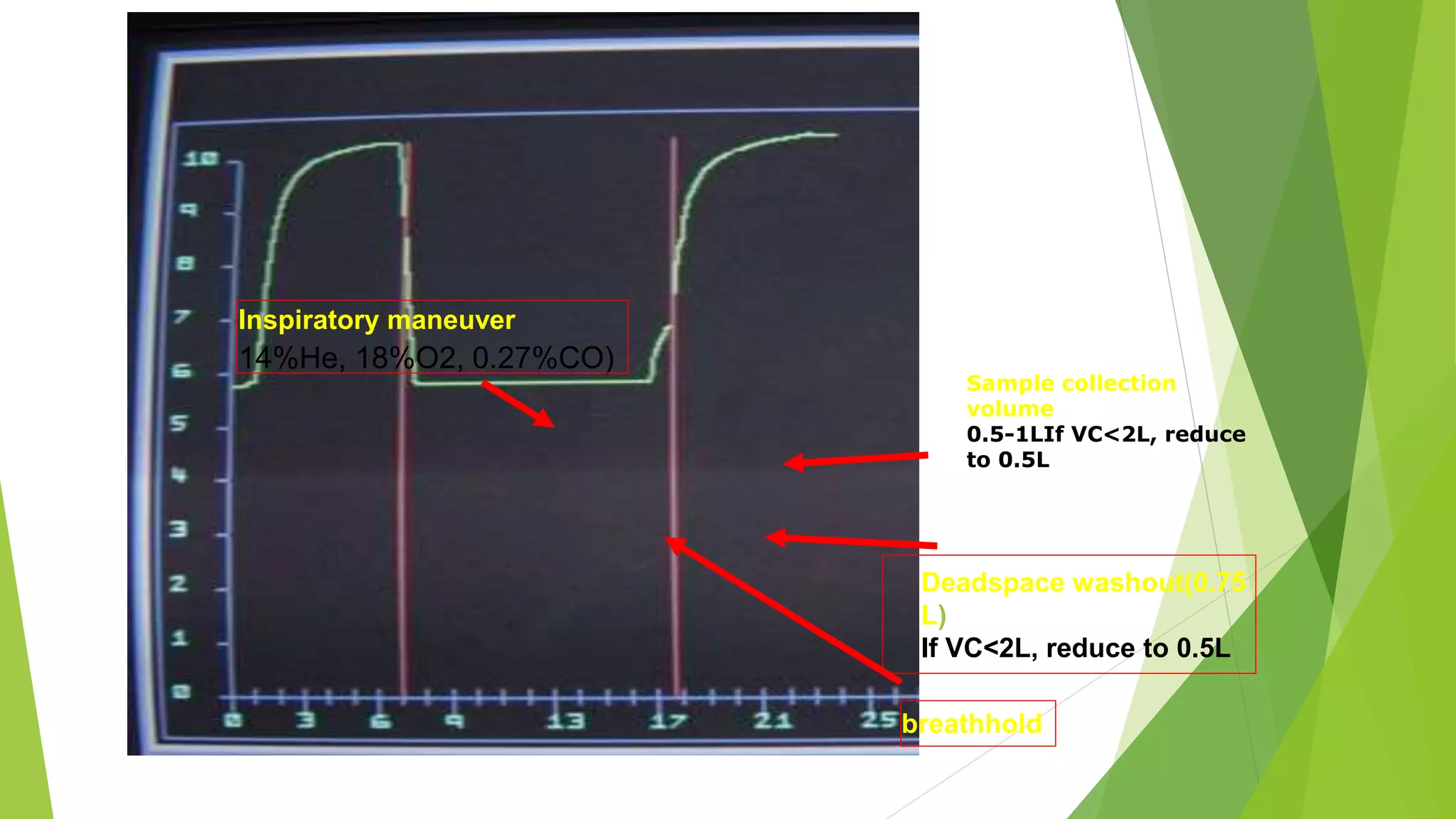
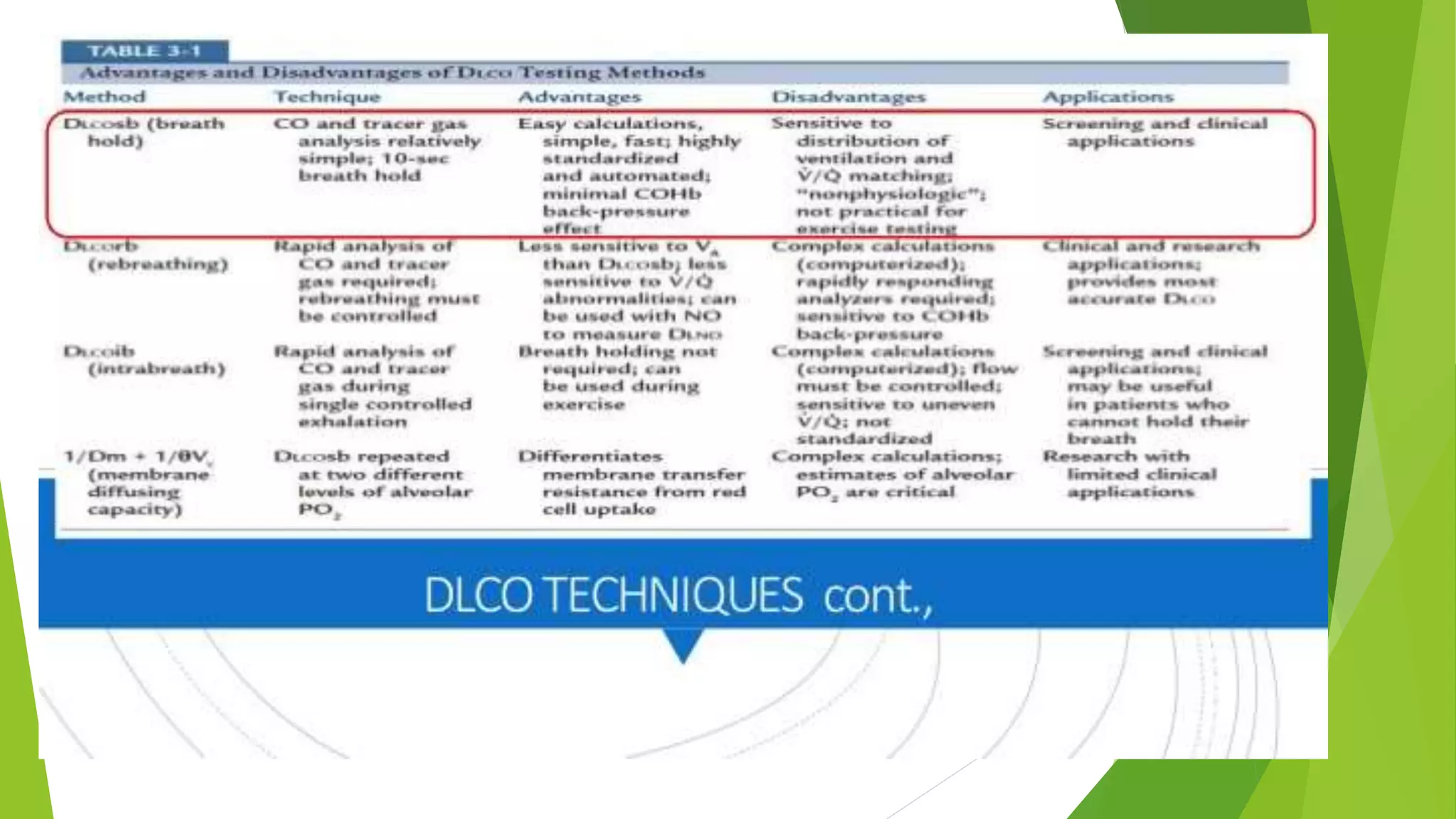
2. It describes the single breath hold method for measuring DLCO, which involves inhaling a gas mixture containing carbon monoxide and exhaling into a collection device to measure gas concentrations.
3. DLCO can be lowered in conditions that decrease the surface area for diffusion like emphysema, or increase the thickness of the alveolar capillary membrane like interstitial lung diseases.