PULMONARY FUNCTION TESTS
STANDARDPFT`S
• SPIROMETRY( including flow
vol loop)
• LUNG VOLUMES TEST`S
• DLCO
SPECIALISED PFT`S
• EXERCISE OXIMETRY
• 6 MINUTE WALK TEST
3.
INDICATIONS OF PFT`S:
⮚Evaluationof case with signs and symptoms suggestive of pulmonary
disease
⮚Monitoring patients with known pulmonary disease for progression
and respone to treatment
⮚Assess pre operative risk
⮚ To Detect pulmomary function abnormality in predisposed individual
( eg:occupational exposure, neuromuscular,chestwall or upper airway)
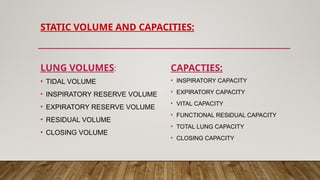
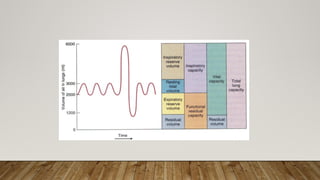
DYNAMIC CAPACITIES ANDVOLUMES:
• Time dependent
• The subject is asked to take deep inspiration followed by fast and
forceful expiration for 6 sec –FVC (forced vital capacity)
• Fast ,forceful expiration in first second is FEV1 ( forced expiratory
volume in 1st
second)
• FEV1/FVC ratio: Tiffneau index
8.
SPIROMETRY
• Spirometer measuresairflow during inspiration or expiration
• Spirometry is recorded graphically and numerically
• Technique :sitting or standing
• Precautions :
✔Avoid smoking 1 hr prior to test
✔Avoid Alcohol 4 hrs prior to test
✔Avoid Vigrous exercise ½ hr prior to test
✔Avoid large meal within 2 hrs of test
✔Avoid clothes which restrict chest and abdominal expansion
9.
SPIROMETRY :
Spirometry manuevers:
⮚Expiratory type
⮚ Inspiratory and expiratory type
Graphically recorded as:
1) Vol v/s time
2) Flow rate v/s volume
- Flow volume curve – when only expiratory flow rate is recorded
- Flow volume loop – when inspiratory flow is also recorded
10.
VALUES MEASURED BYSPIROMETERY
• Major
• FEV
• FVC
• FEV1/FVC ratio
• Flow volume loop
• Minor
• Peak expiratory flow rate
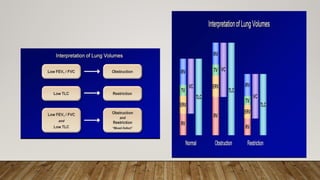
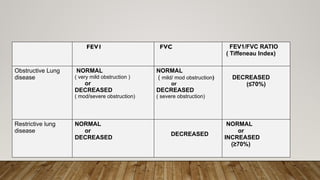
FEV1 FVC FEV1/FVCRATIO
( Tiffeneau Index)
Obstructive Lung
disease
NORMAL
( very mild obstruction )
or
DECREASED
( mod/severe obstruction)
NORMAL
( mild/ mod obstruction)
or
DECREASED
( severe obstruction)
DECREASED
(≤70%)
Restrictive lung
disease
NORMAL
or
DECREASED
DECREASED
NORMAL
or
INCREASED
(≥70%)
14.
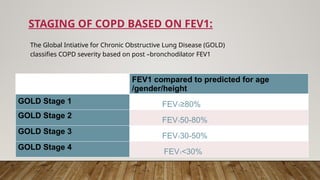
STAGING OF COPDBASED ON FEV1:
The Global Intiative for Chronic Obstructive Lung Disease (GOLD)
classifies COPD severity based on post –bronchodilator FEV1
FEV1 compared to predicted for age
/gender/height
GOLD Stage 1 FEV1≥80%
GOLD Stage 2
FEV150-80%
GOLD Stage 3
FEV130-50%
GOLD Stage 4
FEV1<30%
15.
PFT`S USED TOMEASURE FRC :
• HELIUM DILUTION
• NITROGEN WASHOUT
• BODY PLETHYSMOGRAPHY
• RADIOGRAPHIC MEASURMENTS (CHEST X RAY OR CT)
Gas Dilution Techniques
}
16.
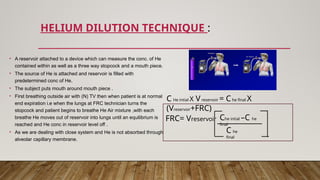
HELIUM DILUTION TECHNIQUE:
C He intial X Vreservoir = Che final X
(Vreservoir+FRC)
FRC= Vreservoir Che intial –C he
final
C he
final
• A reservoir attached to a device which can measure the conc. of He
contained within as well as a three way stopcock and a mouth piece.
• The source of He is attached and reservoir is filled with
predetermined conc of He.
• The subject puts mouth around mouth piece .
• First breathing outside air with (N) TV then when patient is at normal
end expiration i.e when the lungs at FRC technician turns the
stopcock and patient begins to breathe He Air mixture ,with each
breathe He moves out of reservoir into lungs until an equilibrium is
reached and He conc in reservoir level off .
• As we are dealing with close system and He is not absorbed through
alveolar capillary membrane.
17.
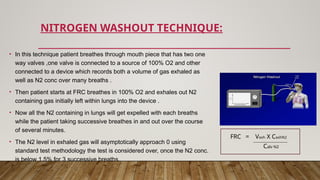
NITROGEN WASHOUT TECHNIQUE:
•In this technique patient breathes through mouth piece that has two one
way valves ,one valve is connected to a source of 100% O2 and other
connected to a device which records both a volume of gas exhaled as
well as N2 conc over many breaths .
• Then patient starts at FRC breathes in 100% O2 and exhales out N2
containing gas initially left within lungs into the device .
• Now all the N2 containing in lungs will get expelled with each breaths
while the patient taking successive breathes in and out over the course
of several minutes.
• The N2 level in exhaled gas will asymptotically approach 0 using
standard test methodology the test is considered over, once the N2 conc.
is below 1.5% for 3 successive breaths.
Calv N2
FRC = Vexh X CexhN2
18.
BODY PLETHYSMOGRAPHY:
• Bestmethod
• Based on boyle`s law
• Measures :
⮚RV
⮚FRC
⮚TLC
Pmi X Vli =PMf X [ VLi + V ]
P –
pressure
V- volume
i- intial
f- final
L-lung
19.
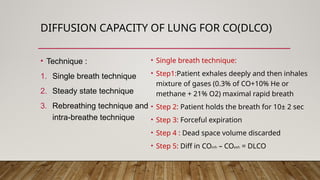
DIFFUSION CAPACITY OFLUNG FOR CO(DLCO)
• Technique :
1. Single breath technique
2. Steady state technique
3. Rebreathing technique and
intra-breathe technique
• Single breath technique:
• Step1:Patient exhales deeply and then inhales
mixture of gases (0.3% of CO+10% He or
methane + 21% O2) maximal rapid breath
• Step 2: Patient holds the breath for 10± 2 sec
• Step 3: Forceful expiration
• Step 4 : Dead space volume discarded
• Step 5: Diff in COinh – COexh = DLCO
20.
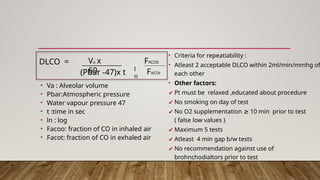
• Va :Alveolar volume
• Pbar:Atmospheric pressure
• Water vapour pressure 47
• t :time in sec
• ln : log
• Facoo: fraction of CO in inhaled air
• Facot: fraction of CO in exhaled air
• Criteria for repeatiability :
• Atleast 2 acceptable DLCO within 2ml/min/mmhg of
each other
• Other factors:
✔ Pt must be relaxed ,educated about procedure
✔ No smoking on day of test
✔ No O2 supplementation 10 min prior to test
≥
( false low values )
✔ Maximum 5 tests
✔ Atleast 4 min gap b/w tests
✔ No recommendation against use of
brohnchodialtors prior to test
(Pbar -47)x t
DLCO = Va x
60 l
n
FACO0
FACOt
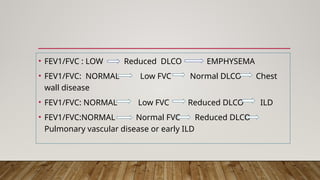
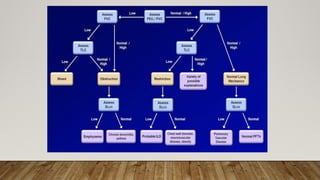
• FEV1/FVC :LOW Reduced DLCO EMPHYSEMA
• FEV1/FVC: NORMAL Low FVC Normal DLCO Chest
wall disease
• FEV1/FVC: NORMAL Low FVC Reduced DLCO ILD
• FEV1/FVC:NORMAL Normal FVC Reduced DLCO
Pulmonary vascular disease or early ILD
23.
CLASSIFACTION AND SEVERITYOF DLCO REDUCTIONS:
• Normal: >75% of predicted , upto140
• Mild decrease :60% to 74%
• Moderate decrease : 40% to 59%
• Severe decrease : < 40%
26.
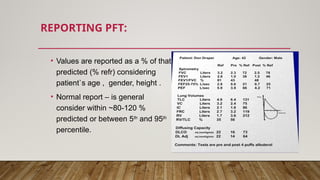
REPORTING PFT:
• Valuesare reported as a % of that
predicted (% refr) considering
patient`s age , gender, height .
• Normal report – is general
consider within ~80-120 %
predicted or between 5th
and 95th
percentile.
27.
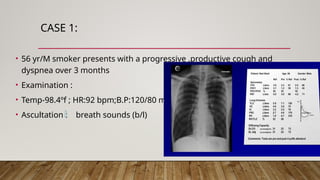
CASE 1:
• 56yr/M smoker presents with a progressive ,productive cough and
dyspnea over 3 months
• Examination :
• Temp-98.4ºf ; HR:92 bpm;B.P:120/80 mm hg
• Ascultation : breath sounds (b/l)
28.
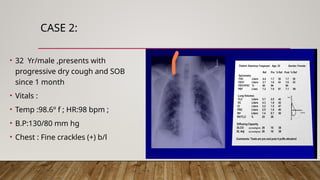
CASE 2:
• 32Yr/male ,presents with
progressive dry cough and SOB
since 1 month
• Vitals :
• Temp :98.6º f ; HR:98 bpm ;
• B.P:130/80 mm hg
• Chest : Fine crackles (+) b/l
29.
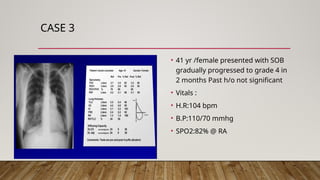
CASE 3
• 41yr /female presented with SOB
gradually progressed to grade 4 in
2 months Past h/o not significant
• Vitals :
• H.R:104 bpm
• B.P:110/70 mmhg
• SPO2:82% @ RA

![BODY PLETHYSMOGRAPHY:
• Best method
• Based on boyle`s law
• Measures :
⮚RV
⮚FRC
⮚TLC
Pmi X Vli =PMf X [ VLi + V ]
P –
pressure
V- volume
i- intial
f- final
L-lung](https://image.slidesharecdn.com/pulmonaryfunctiontests-250621160239-3a282129/85/Pulmonary-function-tests-pptx-respiratory-physiology-18-320.jpg)