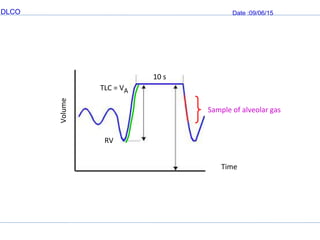
This document provides information on DLCO (diffusion capacity of the lung for carbon monoxide), a test used to evaluate how well oxygen passes from the alveoli into the blood. It describes how DLCO is measured using CO and calculates diffusion capacity based on CO uptake. Factors that influence DLCO levels are also discussed, including hemoglobin concentration, oxygen levels, body position, exercise, and lung volume. Decreased DLCO can indicate obstructive lung diseases, interstitial lung disease, and other conditions, while increased DLCO may be seen in polycythemia and pulmonary hemorrhage. The single-breath method is described as the most common technique for measuring DLCO.