Objectives
• Review theclinical indications of pulmonary function testing
• Recognize a good quality pulmonary function test.
• Recognize the distinct role of lung mechanics tests (spirometry and
lung volumes) and gas exchange tests (DLCO) in the evaluation of
pulmonary impairment.
• Recognize normal patterns of pulmonary function test and flow
volume loops and abnormal patterns of obstructive and restrictive
pulmonary diseases.
• Recognize hyperinflation and air trapping on lung volume testing
• Explain the metacholine challenge test ,its indication and
interpretation
• Explain the six minute walk test (6MWT)
3.
Indications
• Evaluate apatient with a history of lung
disease
• Evaluate a patient at risk for lung disease
• Evaluate a patient with a symptom suggestive
of lung disease (dyspnea, cough,…)
• Assess and monitor a disease and assess the
effect of a therapeutic intervention
• Evaluate preoperative pulmonary risk
4.
Pulmonary function testing
Aidin differentiating obstructive from
restrictive pulmonary disease
• Obstructive pulmonary diseases
• COPD
• Asthma
• Restrictive pulmonary diseases
• Parenchymal diseases or interstitium (such as pulmonary
fibrosis)
• Chest wall diseases or neuromuscular diseases
• Evaluation of Vascular diseases ( pulmonary
hypertension)
How to interpretPFT
• Reference values depend on age, height,
gender , and race
• Use appropriate reference values (obtained
from healthy individuals) with which the
patient’s results are compared
• Results are going to be % of predicted
• Normal range is 80-120% of predicted
Spirometry
• Measures thevolume of air exhaled at specific
time points during a forceful and complete
exhalation after a maximal inhalation
• Measures all components of the VC
• Cannot measure RV
9.
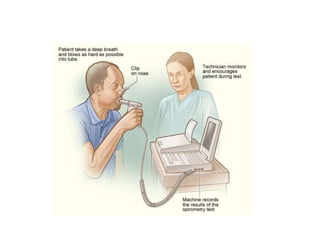
Procedure spirometry
• Patientsare usually seated
• Nose is clipped
• Patient is hooked to a spirometer
• Normal tidal breathing
• The patient exhales completely
• Ask the patient to inspire maximally
• Ask the patient to exhale as hard and as
completely as he can
• Exhalation should last at least 6 seconds
Spirometry
• Most commonlyperformed part of the full
PFT
• FVC (forced vital capacity)
• FEV1 (forced expiratory volume in one second)
• FEV1/FVC ratio
13.
Spirometry
• The forcedvital capacity (FVC) is the maximal
volume of air exhaled with a maximally forced
effort from a position of full inspiration and is
expressed in liters : normal >80% of predicted
• The forced expiratory volume in one second
(FEV1) is the maximal volume of air exhaled in
the first second of a forced exhalation that
follows a full inspiration, expressed in liters :
normal >80% of predicted
• Normally the FEV1 is 80% of the FVC: FEV1/FVC
ratio is > or = to 80%
14.
Spiromerty
• FEV1/FVC:
– Usedto diagnose suspected obstructive pulmonary
disease : <70%
– Most important parameter for detecting airflow limitation
in diseases like asthma and COPD.
• FEV1:
– Most important spirometric variable for assessment of the
severity of airflow obstruction ( mild, moderate or severe)
• Post bronchodilator:
• Administration of short acting β2 agonist (albuterol): Spirometry
should be repeated ten minutes after administration of a
bronchodilator
15.
Spirometry
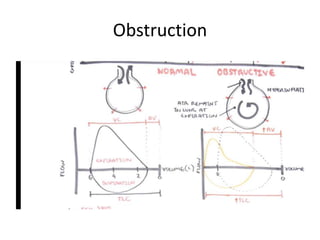
Obstructive pulmonary disease
•FVC normal or decreased <80% ( In severe cases)
• FEV1< 80% because there is resistance to the
expiratory flow (central airways are narrowed)
• FEV1/FVC < 70% predicted FEV1 is more
dramatically reduced
• In a patient with airway obstruction, an increase in the FEV1 of more than
12 % or > 200cc following bronchodilator (βagonist) suggests a significant
acute bronchodilator responsiveness
• (12% is to account for test intervariability)
16.
Spirometry
bronchodilator response
• Inmost patients with asthma, post
bronchodilator testing improve to normal
spirometry values. (reversible airflow
obstruction)
• In COPD you may not see a significant change
in the FEV1 after bronchodilator. If there is a
significant change it never returns to normal
17.
Spirometry
Restrictive pulmonary disease(example
pulmonary fibrosis). All lung volumes and
capacities are reduced.
• FVC < 80%
• FEV1< 80%
• FEV1/FVC > 70% (normal)
18.
Spirometry
• Obstructive
FVC isnormal or decreased
FEV1 is decreased
FEV1/FVC ratio is < 70%
• Restrictive
FVC is decreased
FEV1 is decreased
FEV1/FVC ratio is > 70%
19.
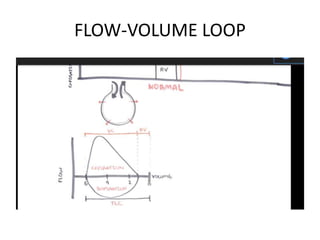
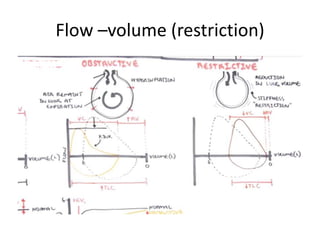
PFT (spirometry)
• Theflow-volume loop is a plot of inspiratory
and expiratory flow (on the Y-axis) against
volume (on the X-axis) during the
performance of maximally forced inspiratory
and expiratory maneuvers
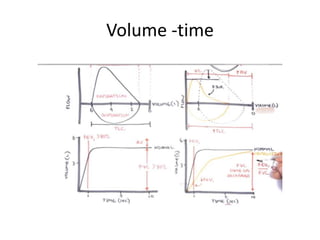
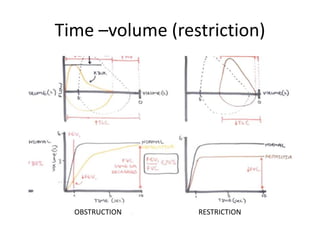
• volume-time spirogram
Recognize a goodspirometry
• Inspection of the flow volume loop
– a sharp peak in the flow curve
– an expiratory duration greater than six seconds
26.
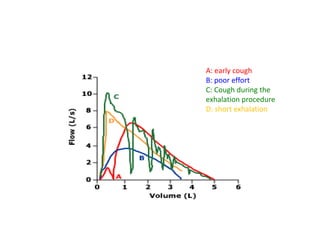
A: early cough
B:poor effort
C: Cough during the
exhalation procedure
D: short exhalation
27.
PFT
When the FVCis decreased, and the FEV/FVC
ratio is normal, then you suspect restrictive
pulmonary disease. It is therefore preferable
to measure TLC , FRC and RV.
It will give us a better idea about the problem.
TLC is what is needed to make the diagnosis of
restrictive pulmonary disease
28.
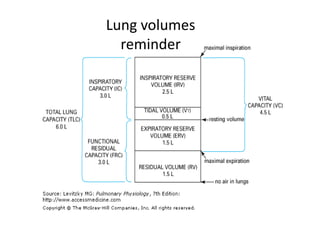
Lung Volumes
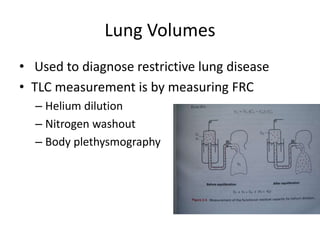
• Usedto diagnose restrictive lung disease
• TLC measurement is by measuring FRC
– Helium dilution
– Nitrogen washout
– Body plethysmography
29.
Lung Volumes
• Functionalresidual capacity (FRC): volume of air
remaining in chest at the end of a tidal volume breath
• Residual volume (RV): volume of air remaining in chest
after maximal exhalation
• Expiratory reserve volume (ERV): volume of air exhaled
from end-tidal volume (FRC) to point of maximal
exhalation (RV)
• FRC=RV+ERV= Resting lung volume
• TLC=FRC+IC
• TLC=RV+VC
Lung volumes inobstructive lung
diseases
RV : may be increased in hyperinflation and air
trapping
RV/TLC ratio:
Increased (> 120% predicted) in airtrapping and
hyperinflation (emphysema)
FRC : may be increased
32.
DLCO
• DLCO measuresthe ability of the lungs to
transfer gas from inhaled air to the red blood
cells in pulmonary capillaries
• Any problem at the alveolar side or the
vascular side is going to affect your DLCO
33.
Physiology
• Reflects propertiesof alveolar-capillary
membrane
• Vgas = (A/T )× (D × (P1 – P2) ).
• The strong affinity of hemoglobin for carbon
monoxide (CO) makes an ideal gas for
measuring properties of alveolar-capillary
membrane (details with Dr Gerges)
34.
Method
• A single-breathmethod, in which the patient quickly
inhales a deep breath of 0.3 percent CO and 10 percent
helium, holds their breath for 10 seconds, and then exhales
quickly
• An alveolar sample of the exhaled gas is then analyzed for
calculation of the dilution of helium and the uptake of CO.
• The rate of disappearance of CO from the alveolar
gas during a 10-second breathhold is obtained by
measuring the inspired and expired [CO] with an
infrared analyzer.
• DLCO is the volume of CO transferred in milliliters per
minute per mm Hg of alveolar partial pressure.
• Normal DLCO: 25ml.min-1.mmHg-1
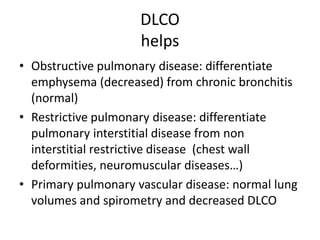
DLCO
helps
• Obstructive pulmonarydisease: differentiate
emphysema (decreased) from chronic bronchitis
(normal)
• Restrictive pulmonary disease: differentiate
pulmonary interstitial disease from non
interstitial restrictive disease (chest wall
deformities, neuromuscular diseases…)
• Primary pulmonary vascular disease: normal lung
volumes and spirometry and decreased DLCO
37.
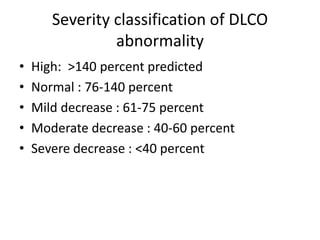
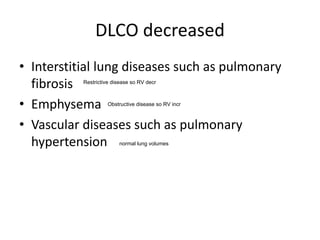
DLCO decreased
• Interstitiallung diseases such as pulmonary
fibrosis
• Emphysema
• Vascular diseases such as pulmonary
hypertension normal lung volumes
Restrictive disease so RV decr
Obstructive disease so RV incr
38.
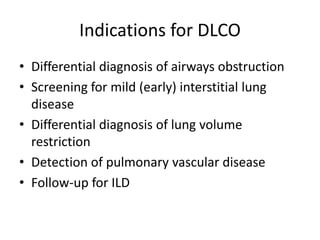
Indications for DLCO
•Differential diagnosis of airways obstruction
• Screening for mild (early) interstitial lung
disease
• Differential diagnosis of lung volume
restriction
• Detection of pulmonary vascular disease
• Follow-up for ILD
39.
AGING
• Healthy never-smokingadults without exposure
to air pollution experience a gradual decline in
lung function.
• The forced expiratory volume in one second
(FEV1) falls approximately 30 mL per year.
• The vital capacity decreases while the residual
volume increases
• The total lung capacity intact.
• The diffusing capacity (DLCO) declines linearly
with age
40.
Bronchoprovocation test
indications
• Accuratediagnosis of asthma
• The patient has symptoms consistent
with asthma but normal pulmonary
function test results and no response to a
bronchodilator
• (asthmatics have often normal PFT
between exacerbations)
41.
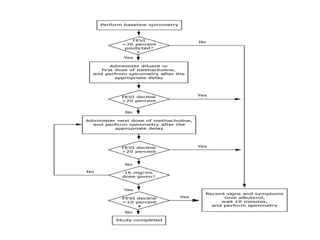
Methacholine challenge test
•Cholinergic (parasympathomimetic) synthetic analogue
of acetylcholine. The drug stimulates muscarinic,
postganglionic parasympathetic receptors, which
results in smooth muscle contraction of the airways
and increased tracheobronchial secretions.
• A series of methacholine chloride solutions are
prepared, ranging from approximately 0.03 mg/mL (the
most dilute) to 16 mg/mL (the most concentrated).
• Given by inhalation
• Contraindicated in patients with evidence wheezing
and a decreased FEV1< 60% predicted
43.
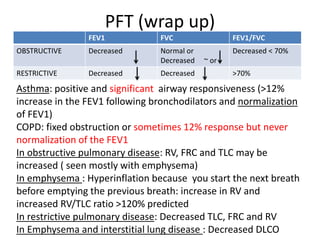
PFT (wrap up)
FEV1FVC FEV1/FVC
OBSTRUCTIVE Decreased Normal or
Decreased ~ or
Decreased < 70%
RESTRICTIVE Decreased Decreased >70%
Asthma: positive and significant airway responsiveness (>12%
increase in the FEV1 following bronchodilators and normalization
of FEV1)
COPD: fixed obstruction or sometimes 12% response but never
normalization of the FEV1
In obstructive pulmonary disease: RV, FRC and TLC may be
increased ( seen mostly with emphysema)
In emphysema : Hyperinflation because you start the next breath
before emptying the previous breath: increase in RV and
increased RV/TLC ratio >120% predicted
In restrictive pulmonary disease: Decreased TLC, FRC and RV
In Emphysema and interstitial lung disease : Decreased DLCO
45.
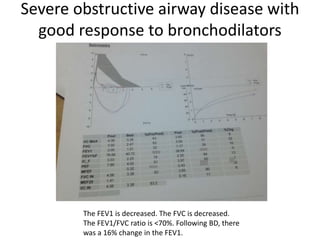
Severe obstructive airwaydisease with
good response to bronchodilators
The FEV1 is decreased. The FVC is decreased.
The FEV1/FVC ratio is <70%. Following BD, there
was a 16% change in the FEV1.
46.
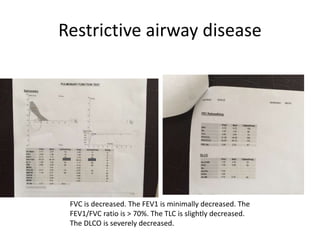
Restrictive airway disease
FVCis decreased. The FEV1 is minimally decreased. The
FEV1/FVC ratio is > 70%. The TLC is slightly decreased.
The DLCO is severely decreased.
48.
Six-minute walk test
•6MWT is a good index of physical function and
response to therapy in patients with COPD,
pulmonary fibrosis and pulmonary arterial
hypertension
• You ask the patient to WALK AS FAST AS
POSSIBLE for 6 minutes on a flat straight
corridor
• DON’T RUN or JOG
49.
Six-minute walk test
•You record baseline oxygen and the heart rate
and at the end of the test
• you calculate the distance walked and you
record
• Healthy subject can typically walk 400 to 700
meters
50.
Six-minute walk test
•The 6MWT is a test that has been used to
assess patients with COPD and pulmonary
hypertension and to follow patients after a
specific therapy.
• It has also been used as an endpoint in studies
evaluating rehabilitation in pulmonary
diseases
51.
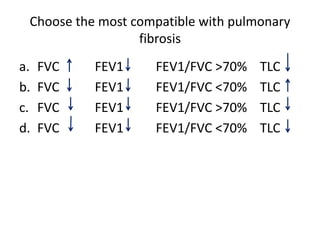
Choose the mostcompatible with pulmonary
fibrosis
a. FVC FEV1 FEV1/FVC >70% TLC
b. FVC FEV1 FEV1/FVC <70% TLC
c. FVC FEV1 FEV1/FVC >70% TLC
d. FVC FEV1 FEV1/FVC <70% TLC
52.
Choose the mostcompatible with
emphysema
a. FVC FEV1 FEV1/FVC >70% RV
b. FVC nl FEV1 FEV1/FVC <70% RV
c. FVC FEV1 FEV1/FVC >70% RV
d. FVC FEV1 FEV1/FVC <70% RV

![Method
• A single-breath method, in which the patient quickly
inhales a deep breath of 0.3 percent CO and 10 percent
helium, holds their breath for 10 seconds, and then exhales
quickly
• An alveolar sample of the exhaled gas is then analyzed for
calculation of the dilution of helium and the uptake of CO.
• The rate of disappearance of CO from the alveolar
gas during a 10-second breathhold is obtained by
measuring the inspired and expired [CO] with an
infrared analyzer.
• DLCO is the volume of CO transferred in milliliters per
minute per mm Hg of alveolar partial pressure.
• Normal DLCO: 25ml.min-1.mmHg-1](https://image.slidesharecdn.com/pulmonaryfunctiontesting2024students-251027211738-cd1971dc/85/Pulmonary-Function-testing-2024-students-pdf-34-320.jpg)