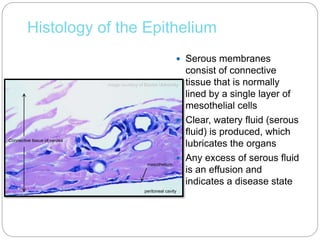
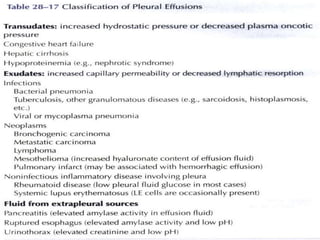
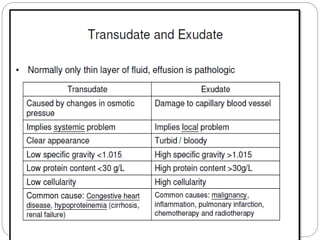
The document discusses effusion cytology. It begins by describing the anatomy of serous cavities and membranes that line them, producing serous fluid. Any excess fluid is an effusion, indicating a pathological process. Effusions can be classified as hydrostatic, infectious, inflammatory, or malignant. Samples are collected and prepared as smears for staining.
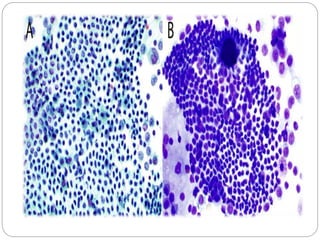
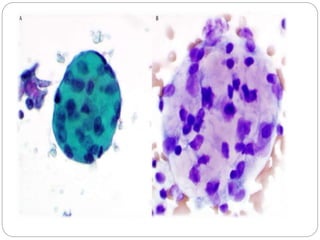
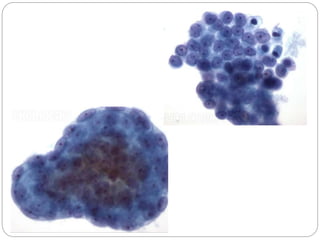
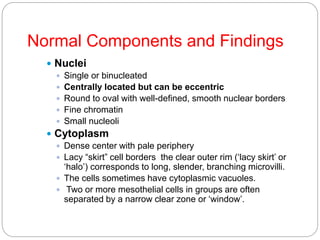
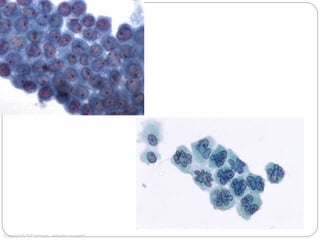
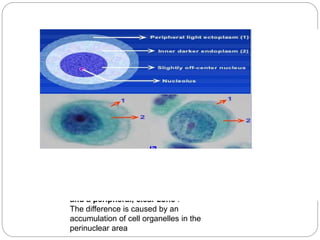
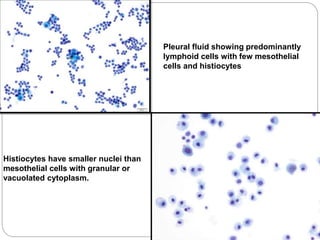
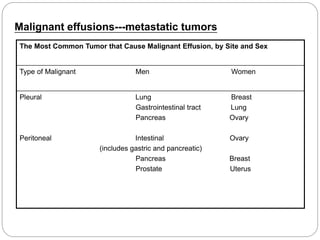
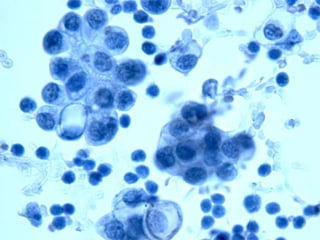
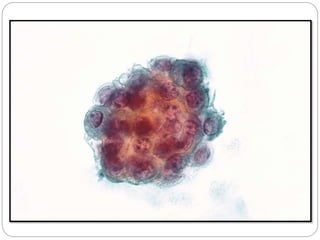
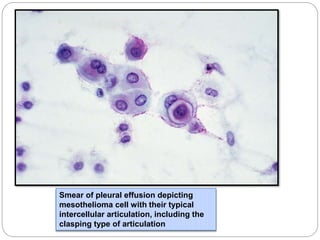
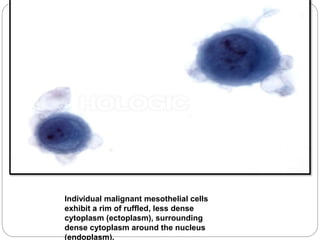
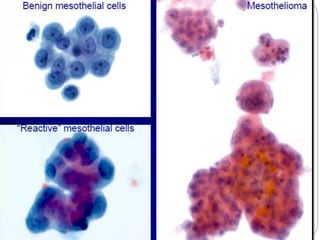
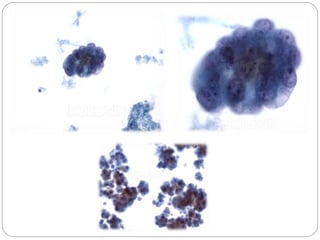
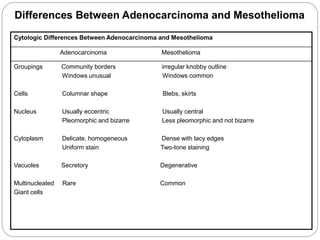
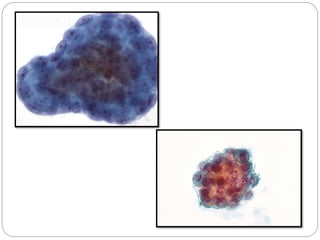
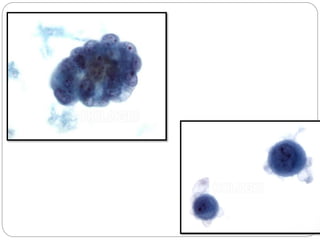
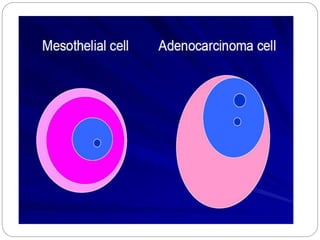
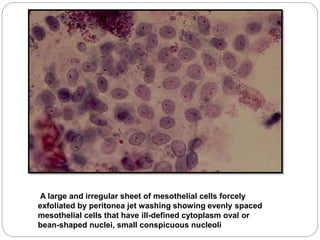
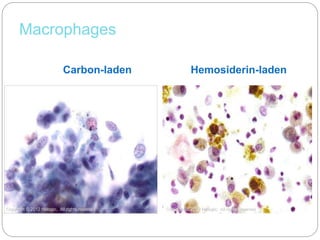
Normal components in effusions include mesothelial cells, histiocytes, lymphocytes, and other inflammatory cells. Reactive mesothelial cells can appear atypical but maintain a uniform appearance. Malignant effusions result from direct extension or metastasis of cancers. Identifying malignant cells involves comparing size, shape and number to determine the primary tumor type and origin. The most