Downloaded 65 times
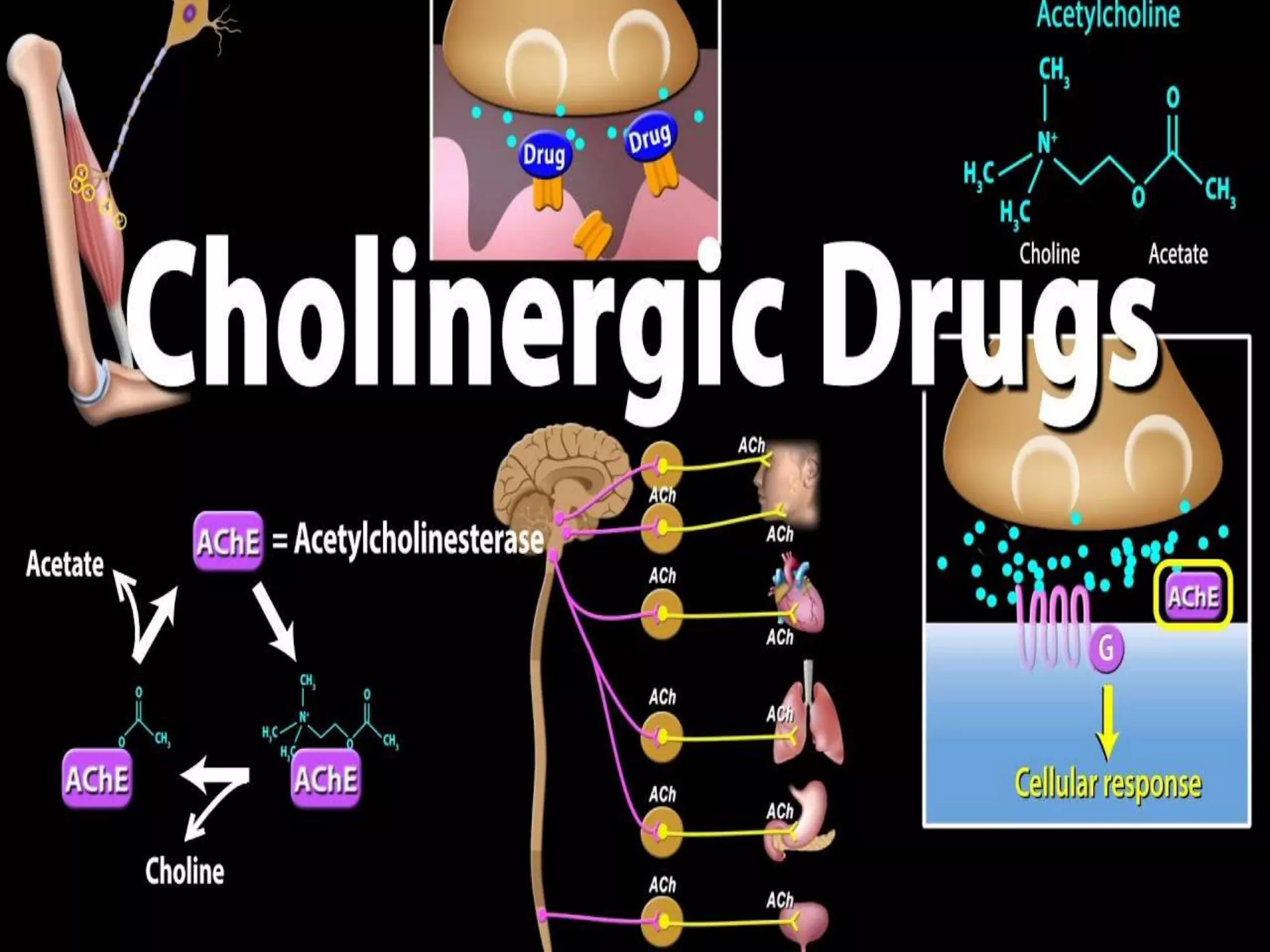

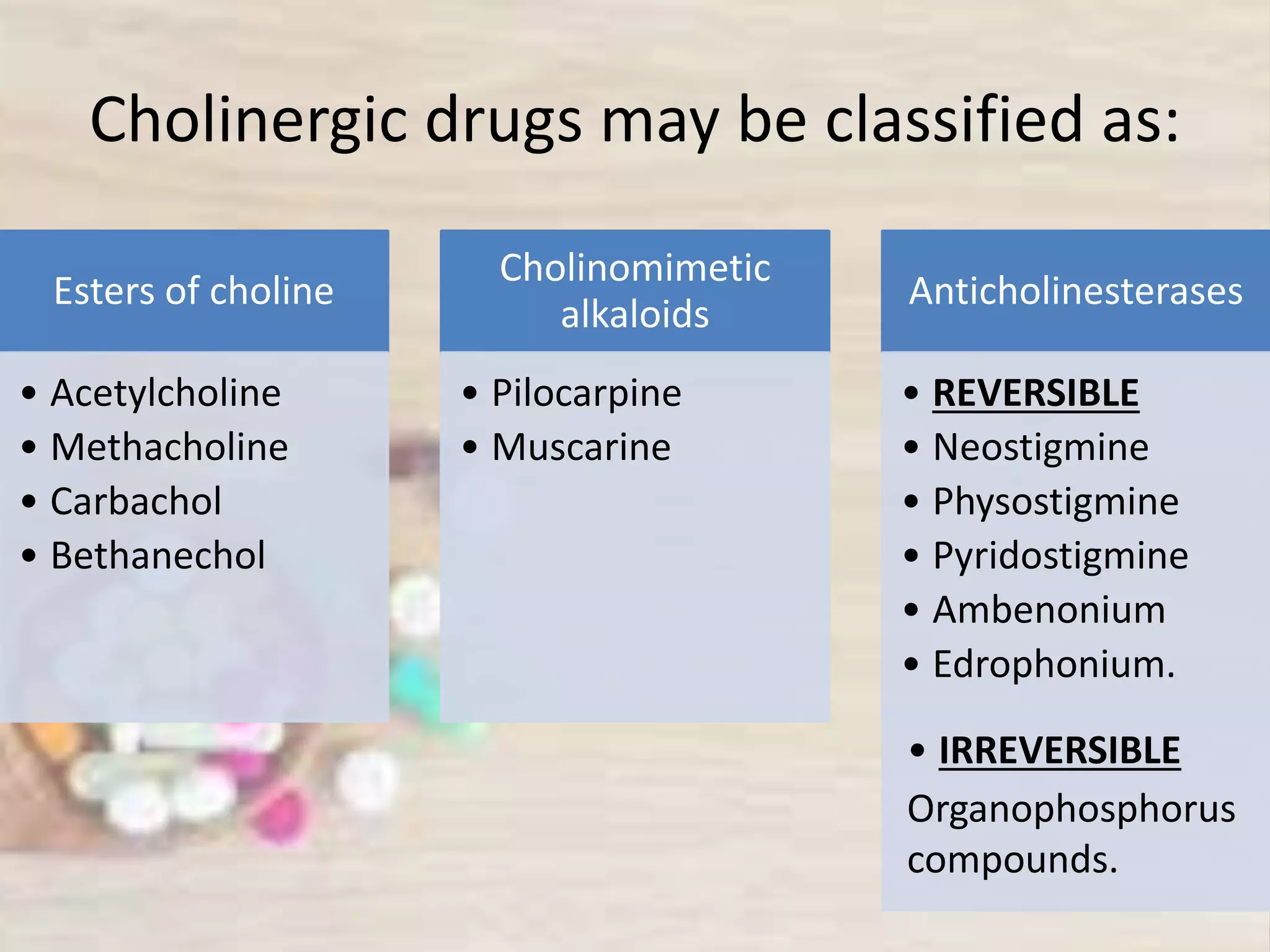





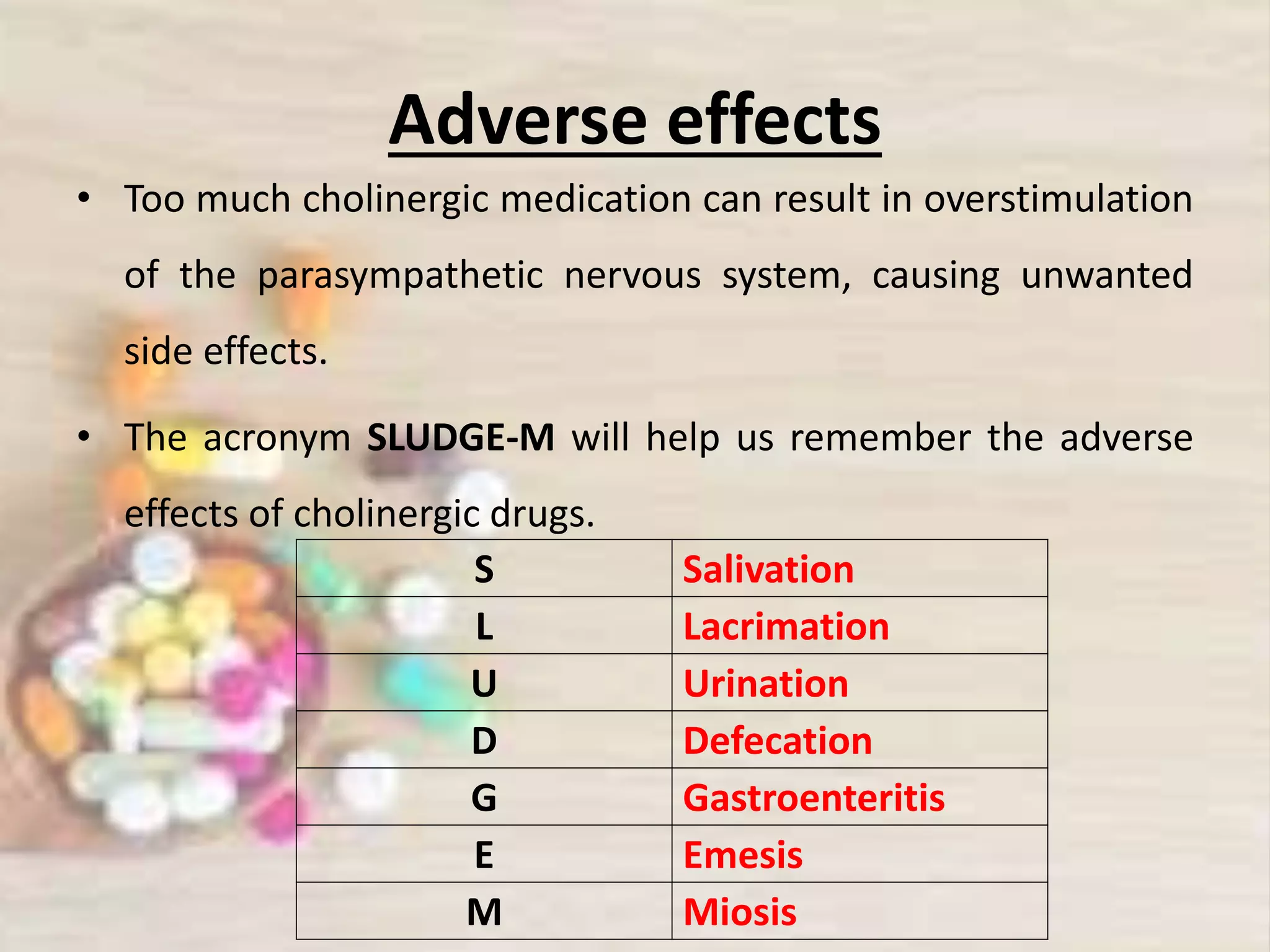





























Cholinergic drugs, or parasympathomimetics, stimulate the parasympathetic nervous system by mimicking the neurotransmitter acetylcholine (ACh). They are categorized into direct-acting drugs, which stimulate cholinergic receptors, and indirect-acting drugs, which inhibit acetylcholinesterase to increase ACh availability. Common uses include treating glaucoma and urinary retention, but there are contraindications and adverse effects, including potential overstimulation of the parasympathetic system.























































































