Downloaded 43 times

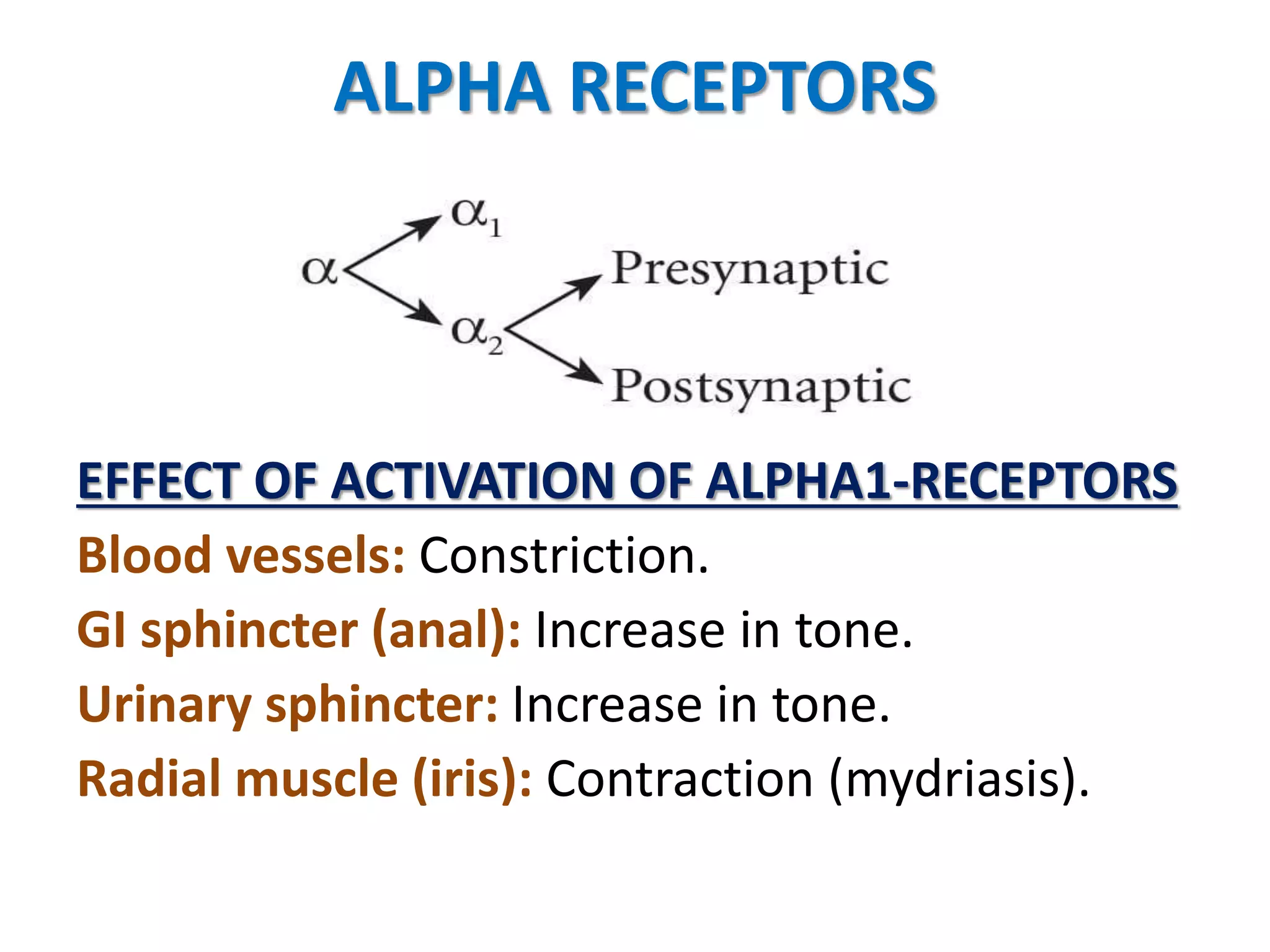
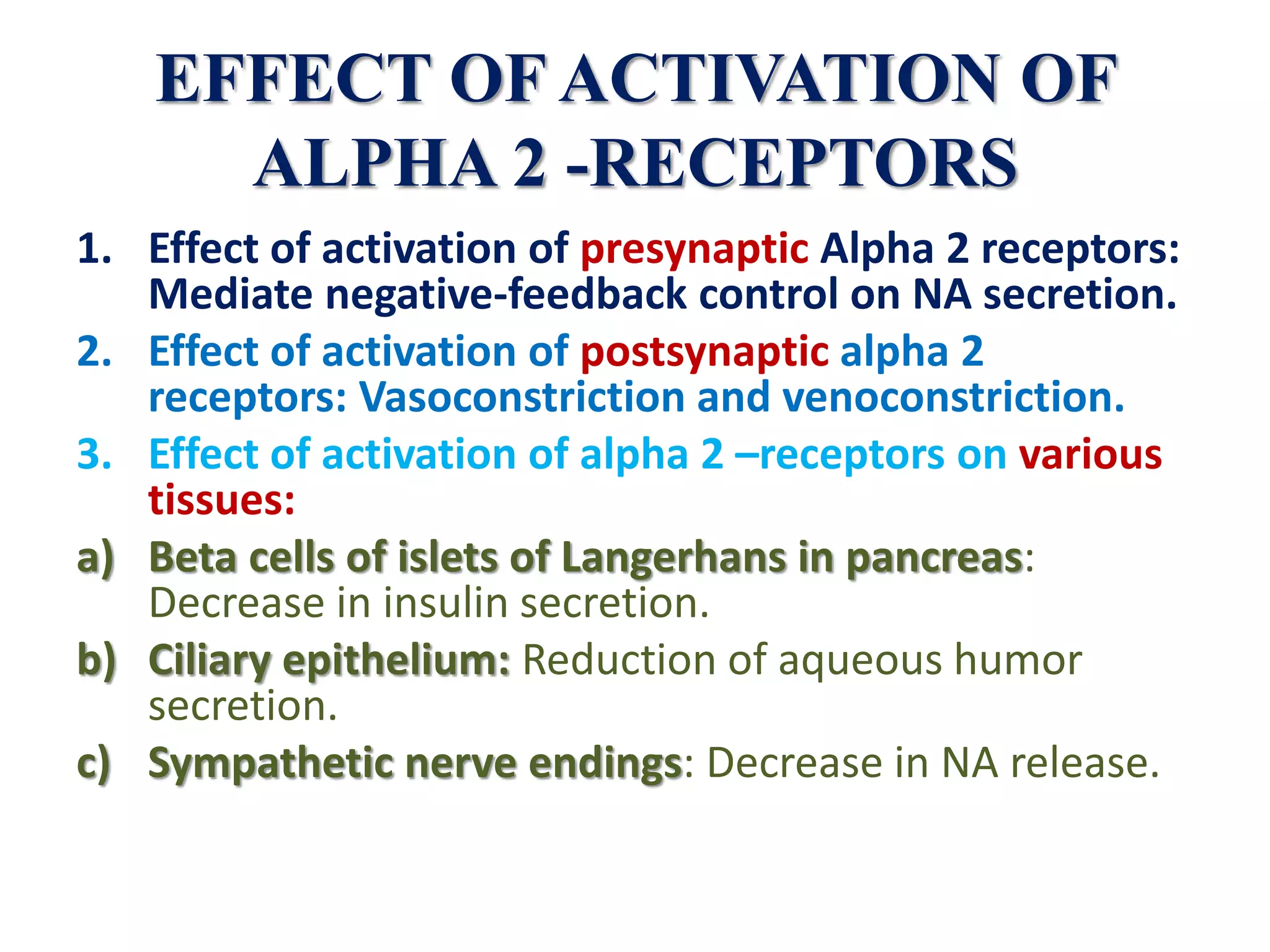

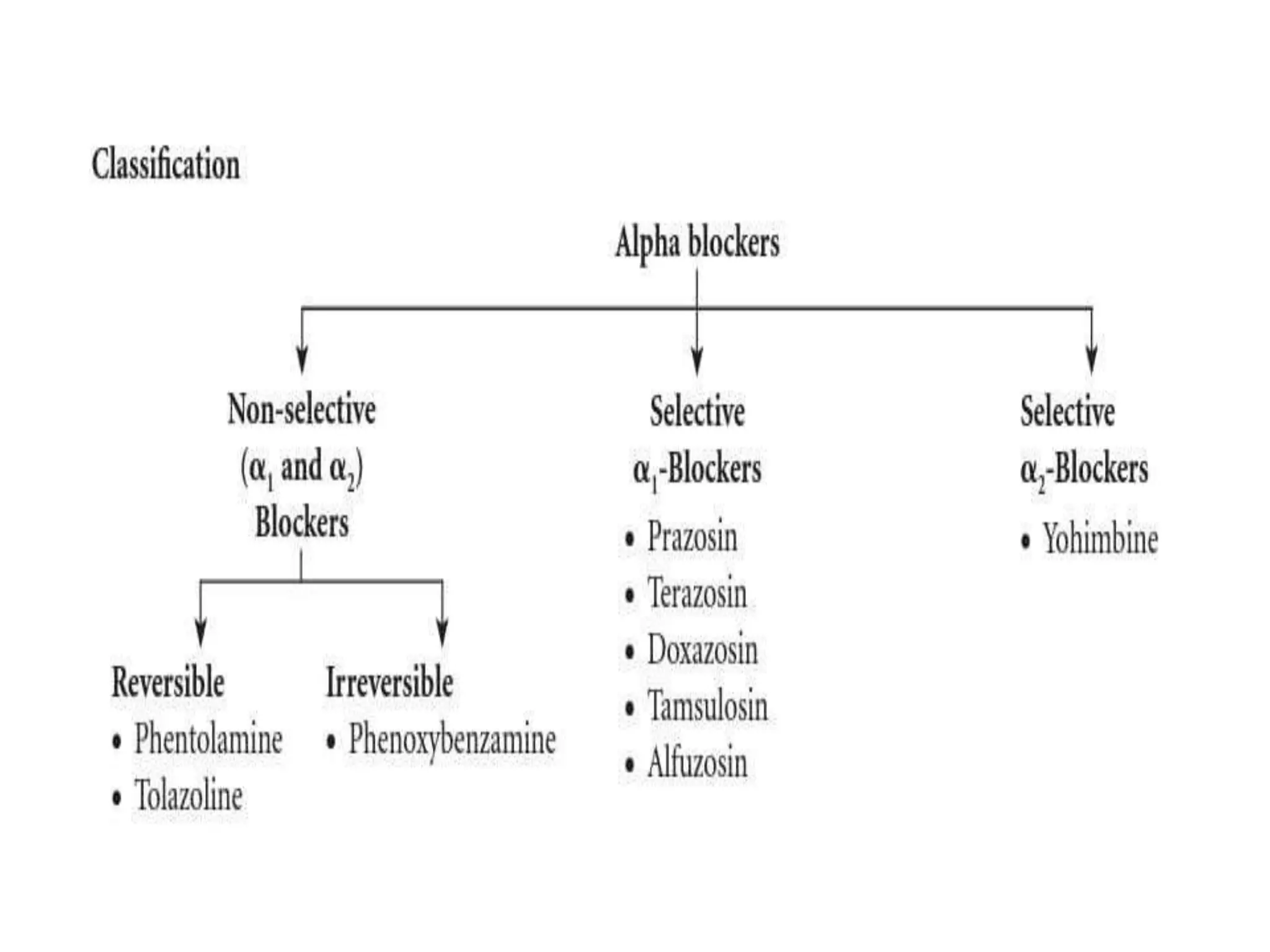





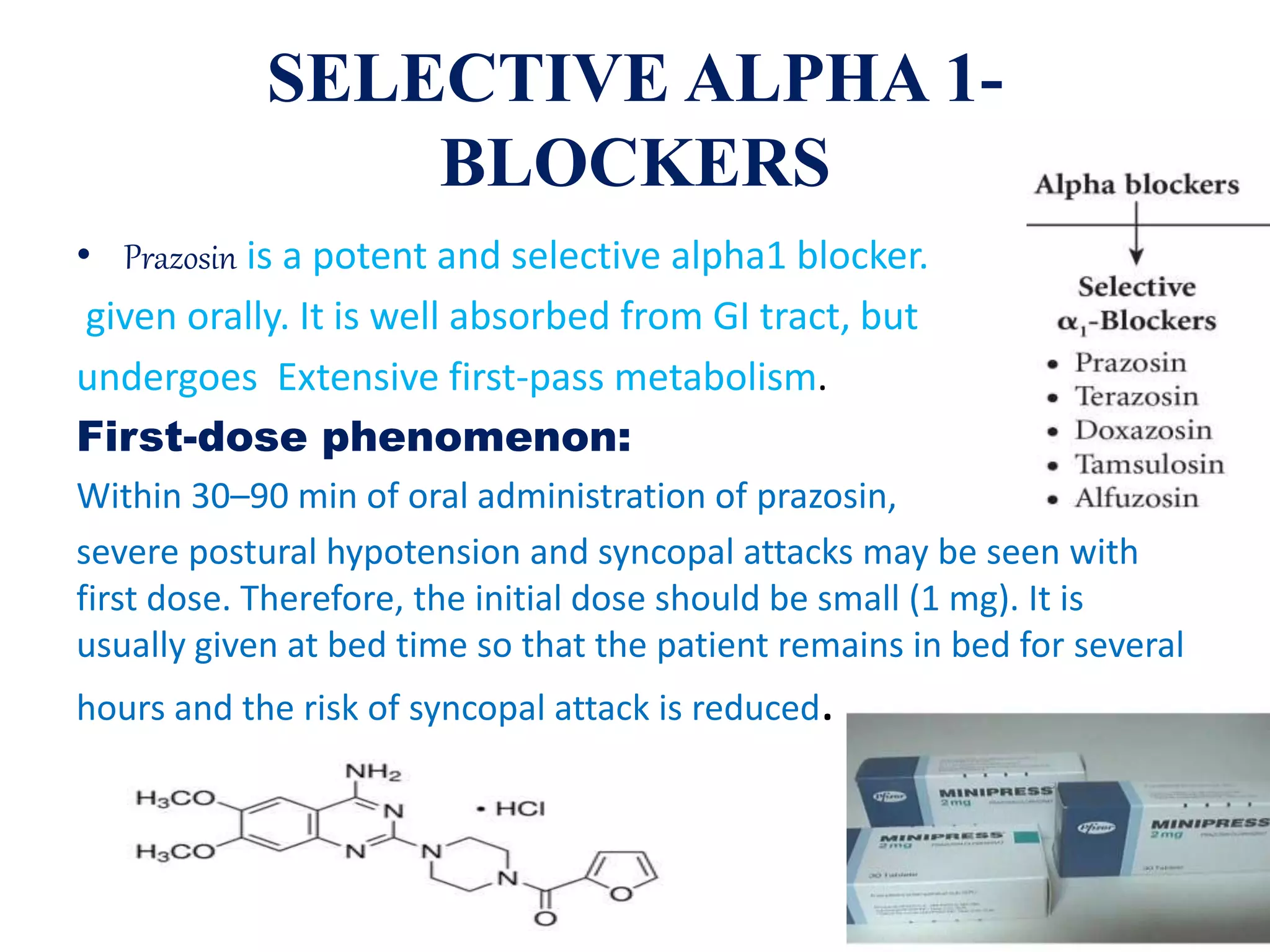

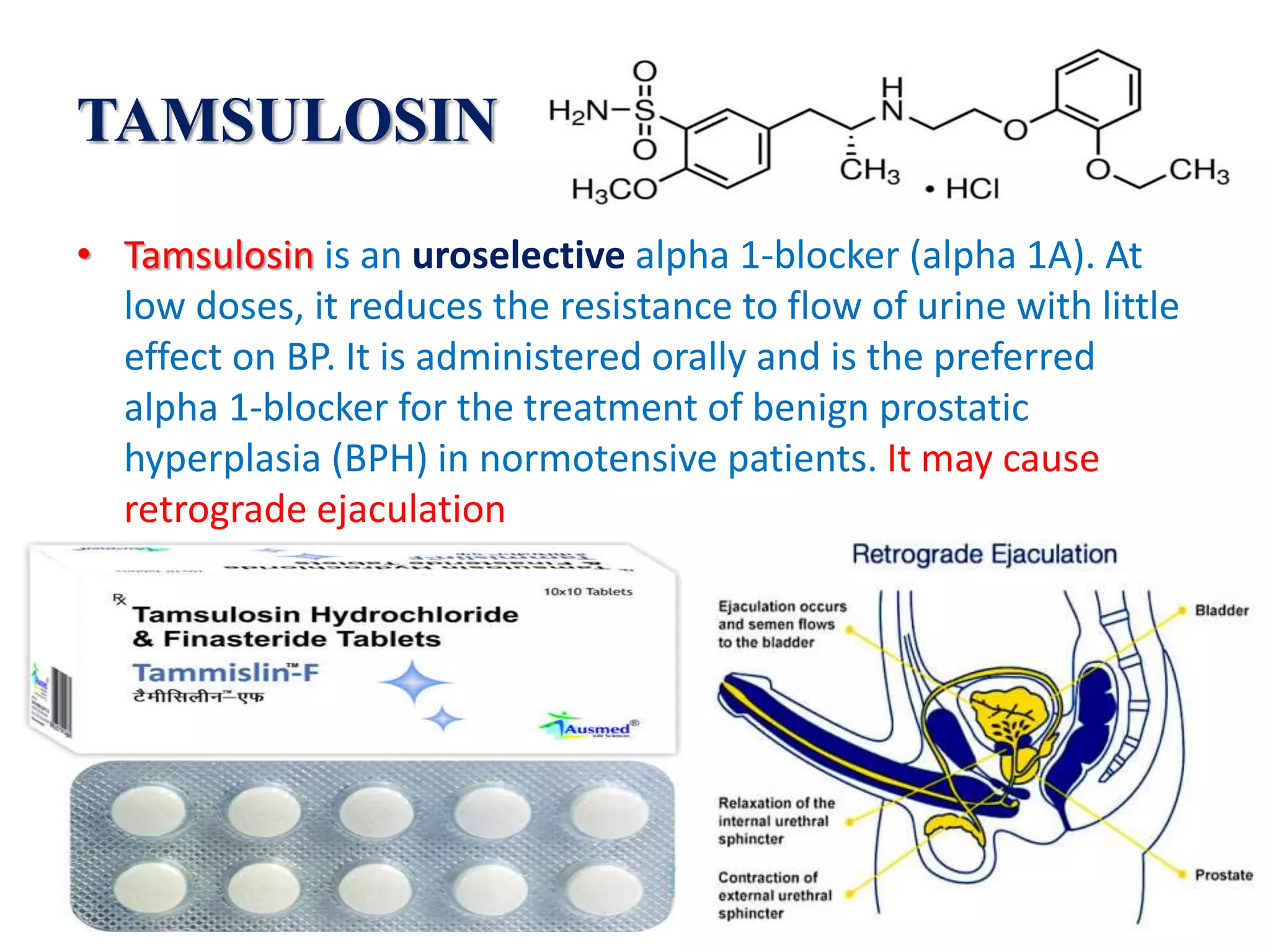



The document discusses alpha receptor blockers, detailing their pharmacological actions, specific medications, and therapeutic uses. It highlights the effects of activation on alpha-receptors, various types of alpha blockers such as phenoxybenzamine and prazosin, and their applications for conditions like pheochromocytoma and benign prostatic hyperplasia. Adverse effects, dosing considerations, and mechanisms of action for multiple blockers are also summarized.























































































