Downloaded 480 times






















































































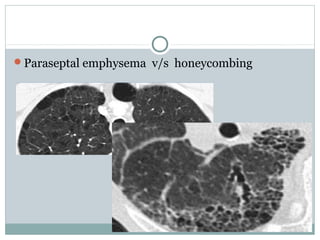



























The document discusses various patterns seen on HRCT scans of the lungs. It begins by describing the basic anatomical structure of the secondary pulmonary lobule. It then discusses numerous findings seen on HRCT scans including interlobular septal thickening, ground glass opacities, nodules, parenchymal opacification, low attenuation areas such as cysts and honeycombing. It also covers emphysema patterns, mosaic perfusion, bronchiectasis and other findings. The document provides details on the appearance and potential causes of each type of finding to aid in radiological interpretation.



































































