Radiological Features of Scimitar Syndrome
•Download as PPTX, PDF•
21 likes•5,682 views

Scimitar syndrome is characterized by a hypoplastic right lung drained by an anomalous vein into the inferior vena cava, known as a scimitar vein. It presents with a partial anomalous pulmonary venous return most commonly on the right side. Associated findings include congenital heart defects, diaphragmatic anomalies, and vertebral anomalies. Radiological imaging plays an important role in diagnosis, with chest x-rays sometimes showing the scimitar vein and reduced lung volume. CT and MRI are useful to precisely map the anomalous pulmonary vein and associated abnormalities.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Radiological Features of Scimitar Syndrome
Similar to Radiological Features of Scimitar Syndrome (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Radiological Features of Scimitar Syndrome
- 1. Radiological imaging of Scimitar Syndrome. Dr/ ABD ALLAH NAZEER. MD.
- 2. Scimitar syndrome, also known as hypogenetic lung syndrome,is characterized by a hypoplastic lung that is drained by an anomalous vein into the systemic venous system. It is a type of partial anomalous pulmonary venous return and is one of several findings in congenital pulmonary venolobar syndrome. Pathology It is essentially a combination of pulmonary hypoplasia and partial anomalous pulmonary venous return (PAPVR). It almost exclusively occurs on the right side. Hemodynamically, there is an a cyanotic left to right shunt. The anomalous vein usually drains into: inferior vena cava: most common right atrium portal vein The aorta frequently perfuses the lung, but the bronchial tree is still connected, and thus the lung is not sequestered.
- 3. Associations congenital heart disease, e.g. ASD, VSD, tetralogy of Fallot, PDA ipsilateral diaphragmatic anomalies, e.g. accessory diaphragm, diaphragmatic hernia localized bronchiectasis horseshoe lung vertebral anomalies, e.g. hemivertebrae genitourinary tract abnormalities pulmonary sequestration Clinical Findings Scimitar syndrome may be diagnosed in infancy because of the associated symptomatic congenital cardiovascular disease (25-50%). Associated congenital cardiac anomalies include: atrial septal defect, ventricular septal defect, patent ductus arteriosus, tetralogy of Fallot, coarctation of the aorta, hypoplasia of the left heart, and various endocardial cushion defects. Some patients may present with hemoptysis and/or recurrent pulmonary infection. Approximately 50% of patients are asymptomatic and diagnosed incidentally on chest radiography acquired for unrelated reasons. Women are slightly more often affected with a female-to-male ratio of 1.4:1.
- 4. Radiographic features The diagnosis is made by transthoracic or transesophageal echocardiography, angiography, or by CT or MR angiography. Plain radiograph Chest radiographic findings are that of a small lung with ipsilateral mediastinal shift, and in one third of cases, the anomalous draining vein may be seen as a tubular structure paralleling the right heart border in the shape of a Turkish sword (“scimitar”). The right heart border may be blurred. Small right lung and hemithorax. Mediastinal shift to the right with dextroversion of the heart. Indistinct right cardiac border Blunted costo phrenic angle Vertically-oriented curved tubular opacity (anomalous draining vein) in right inferior thorax coursing towards right cardiophrenic angle. Diminished right pulmonary vascularity. MDCT / MRI Allows optimal visualization of the anomalous draining vessel and its course and drainage into IVC, hepatic circulation, right atrium, or coronary sinus Non-invasive assessment of left-to-right shunts with velocity-encoded cine MRI
- 5. The right hemithorax is hypoplastic. Also, a tubular structure is seen in the lower right lung, which has the shape of a scimitar; the findings are suggestive of Scimitar's syndrome (pulmonary venolobar syndrome or hypogenetic lung syndrome), a type of partial anomalous pulmonary venous return (PAPVR). The heart is displaced to the right. The left pulmonary artery is very prominent.
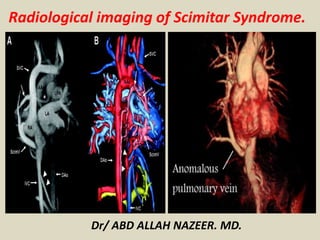
- 9. A chest radiography of a patient with scimitar syndrome showing a left-side anomalous pulmonary vein (Panel A), which was confirmed by magnetic resonance imaging (Panel B).
- 10. Scimitar syndrome. Newborn with tachypnea. A, Frontal chest radiograph demonstrates dextrocardia with decreased aeration of the right lung. B, Subsequent coronal reformatted chest CT image shows shift of the heart into the right side of the chest with the left ventricle (LV) apex to the left and right ventricle (RV) to the right consistent with dextroposition or secondary dextrocardia. C, A posterior coronal reformatted image shows anomalous pulmonary venous drainage of the left lung to the IVC with a scimitar vein (arrow). D, Coronal minimum intensity projection image demonstrates that the right main stem bronchus bifurcates to support two lobes of the lung separated by a single fissure (arrow) consistent with absence of the right upper lobe.
- 11. Baffle obstruction after repair of scimitar syndrome; 24-year-old with exercise intolerance. Coronal maximum intensity projection (A) from MRA demonstrates anomalous pulmonary venous drainage (arrow) of the entire right lung to the IVC. After surgical construction of a baffle to connect the pulmonary venous drainage to the left atrium, coronal maximum intensity projection image from MRA (B) demonstrates complete baffle obstruction (arrow). The baffle also underwent dehiscence, allowing the scimitar vein to connect to the IVC, which is markedly dilated.
- 12. Scimitar syndrome with a hypoplastic right lung.
- 16. Chest radiograph (left) and chest computed tomography (right, A–D) in a 4-day-old boy with scimitar syndrome. Although right lung hypoplasia and shift of the mediastinal structures to the right are well delineated on the chest radiograph, the anomalous pulmonary venous return (“scimitar vein”; black arrowheads) cannot be readily appreciated. The scimitar vein is better appreciated with computed tomography (performed at age 4 days; white arrowheads), which also confirmed right lung hypoplasia and mild compression of the right lower lobe. Additional partial anomalous pulmonary venous return vessels were not identified, possibly owing to the small anatomic scale at that age and a lack of information on blood flow direction.
- 18. A 78-yr-old female with history of chronic dyspnea and scimitar syndrome. Contrast enhanced computed tomography (CT) was acquired with 3-mm sections. a) Axial CT image at the level of the left atrium shows absence of left upper pulmonary vein (arrow). b) Axial CT image at the level of the right inferior pulmonary vein (arrow) shows enlargement of the vein that enters the right atrium (star). c) Coronal multiplanar reformation shows the enlargement and abnormal position of the right pulmonary vein (arrow) and the continuity with the right atrium (star). d) Three-dimensional surface shaded display view in a coronal projection of the malformation (arrow).
- 19. Scimitar syndrome, (a) Chest CT shows hypoplasia of the right lung, mediastinal shift and abnormal vascularization of the right lung; (b) MDCT chest showing small right pulmonary artery (white arrow); (c) MDCT chest showing systemic arterial supply of the right lung; (d) MDCT chest showing absence of right pulmonary venous drainage to left atrium.
- 20. Scimitar syndrome in a 53-year-old man. Coronal and sagittal maximum-intensity-projection reformatted image shows a large anomalous vein draining into the inferior vena cava, below the level of the right diaphragm (*).
- 21. Multislice, single-phase, fast imaging with steady-state precession (TrueFISP) sequence on coronal (A and B) and axial (C and D) planes shows an anomalous vessel in the right lung (arrows) connected to the inferior vena cava.
- 22. A, Maximum-intensity projection of the phase-contrast angiogram in sagittal oblique direction as seen from 30° left anterior oblique view. In addition to the pronounced scimitar vein (ScimV), the hypoplastic right pulmonary artery (*), an additional partial anomalous pulmonary venous return vein in the right upper lobe (open white arrow), and the anomalous systemic artery from the celiac trunk to the right lower lung (white arrowheads) can be appreciated. B, Posterior view of segmented PC- VIPR angiography data with color-shaded surface display. For detailed understanding and ready apprehension, the oxygenized arterial (red), oxygenized partial anomalous pulmonary venous return (pink), deoxygenized venous and right ventricular (blue) structures, and portal venous system (yellow) were color-coded. SVC indicates superior vena cava; AAo, ascending aorta; LPA, left pulmonary artery; LA, left atrium; RA, right atrium; IVC, inferior vena cava; and DAo, descending aorta.
- 23. MRI of Partial Anomalous Pulmonary Venous Return - Scimitar Syndrome
- 24. Scimitar syndrome: multislice computer tomography with three-dimensional reconstruction.
- 25. Thank You.