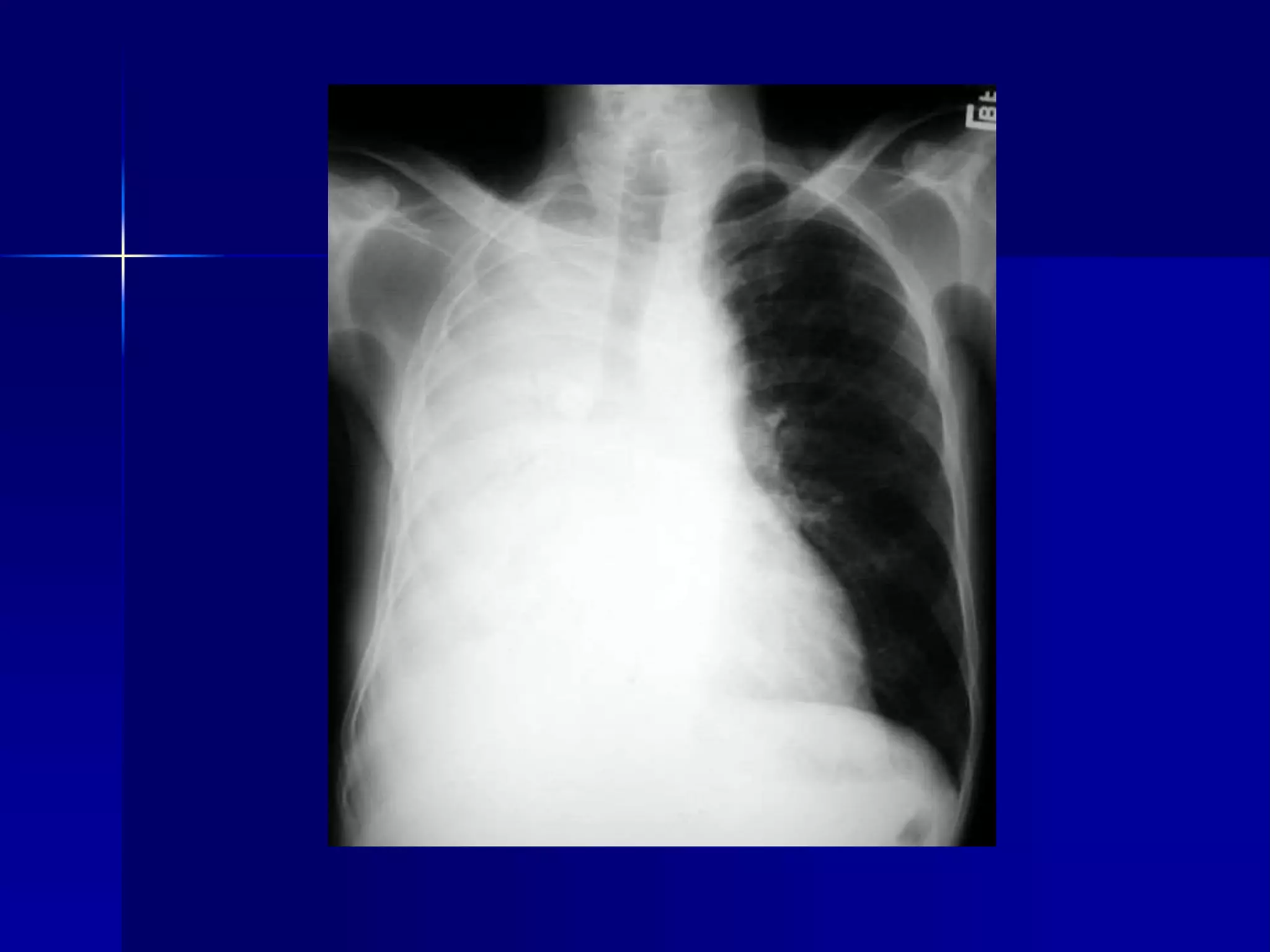
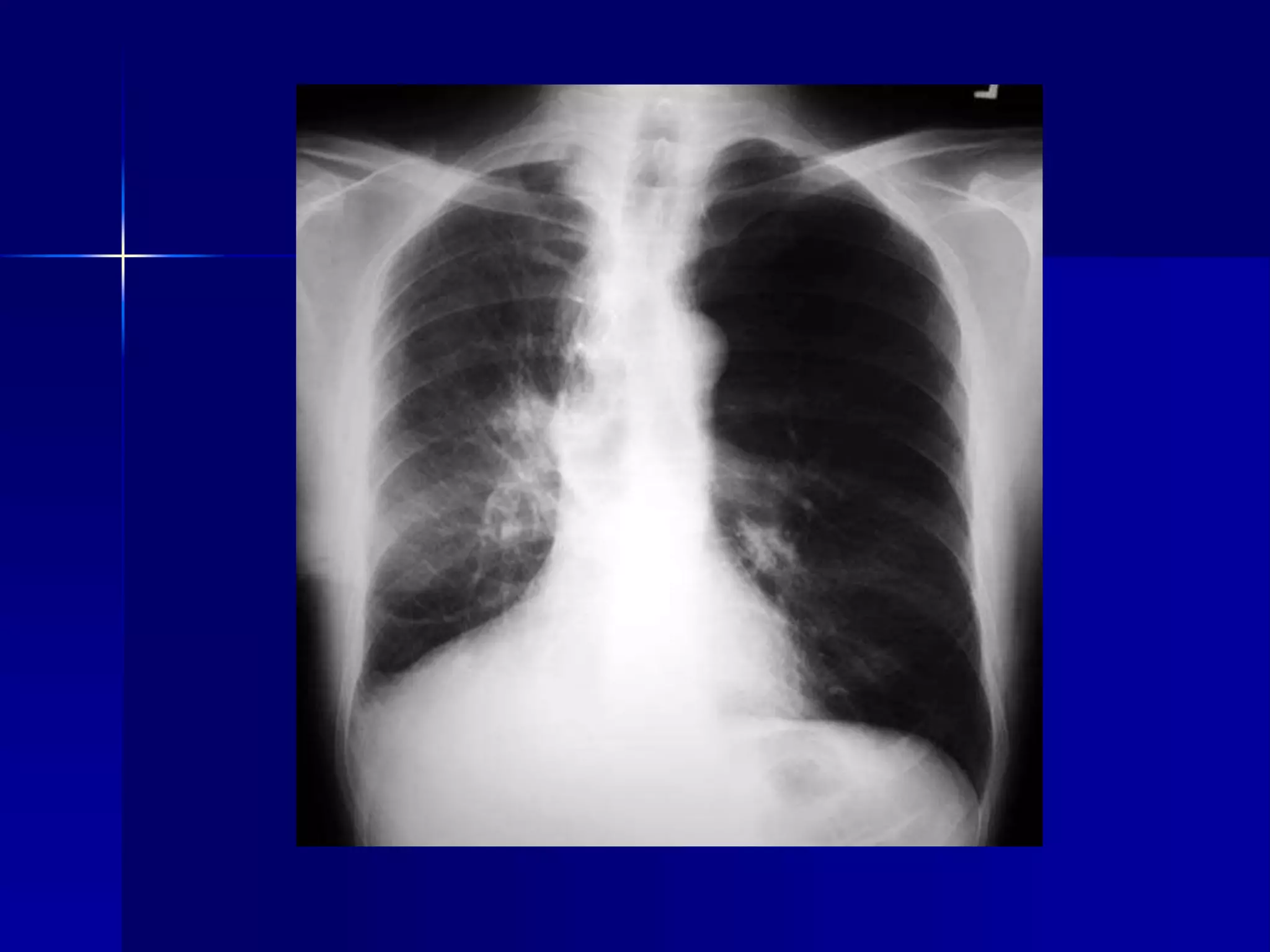
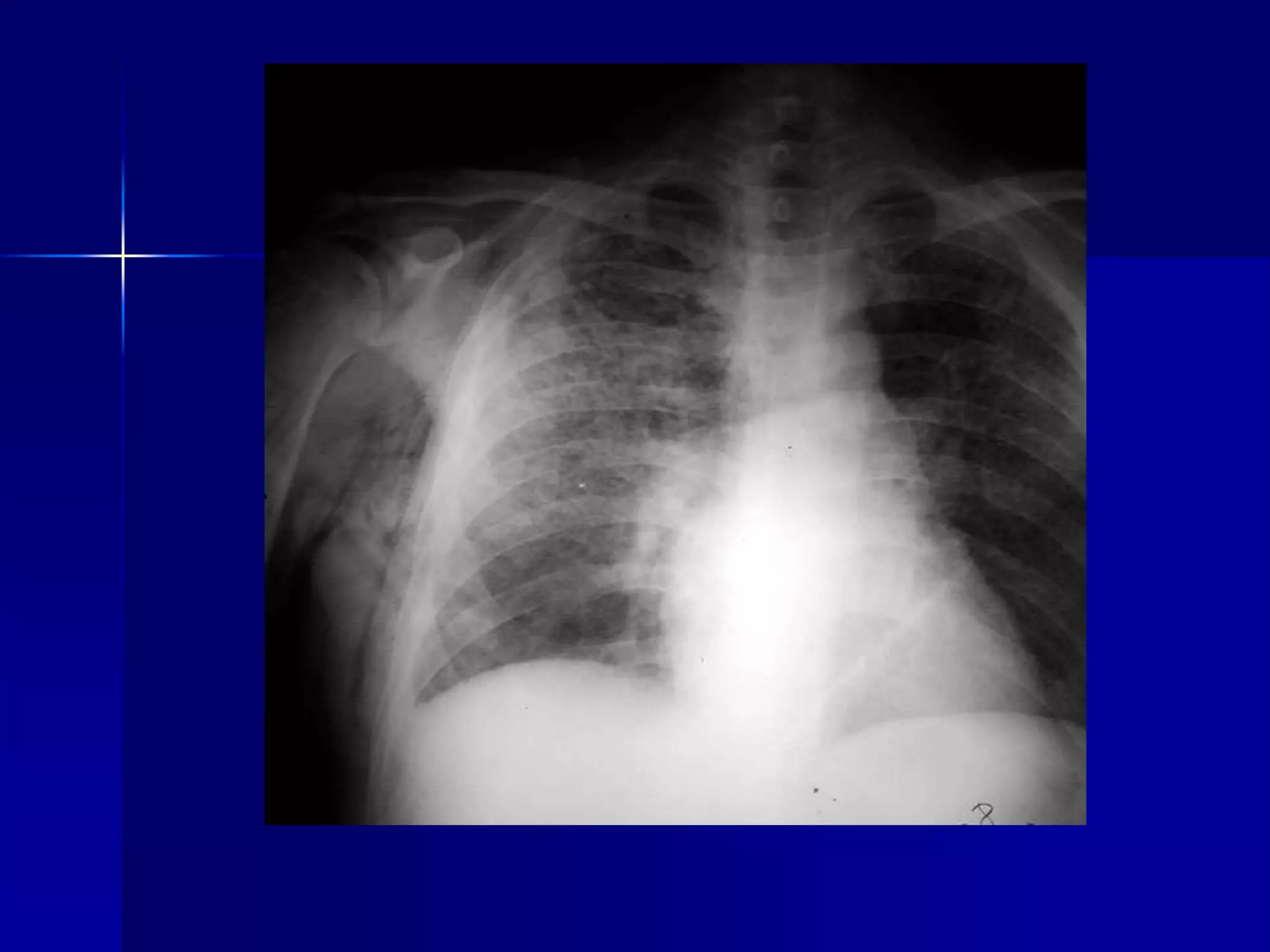
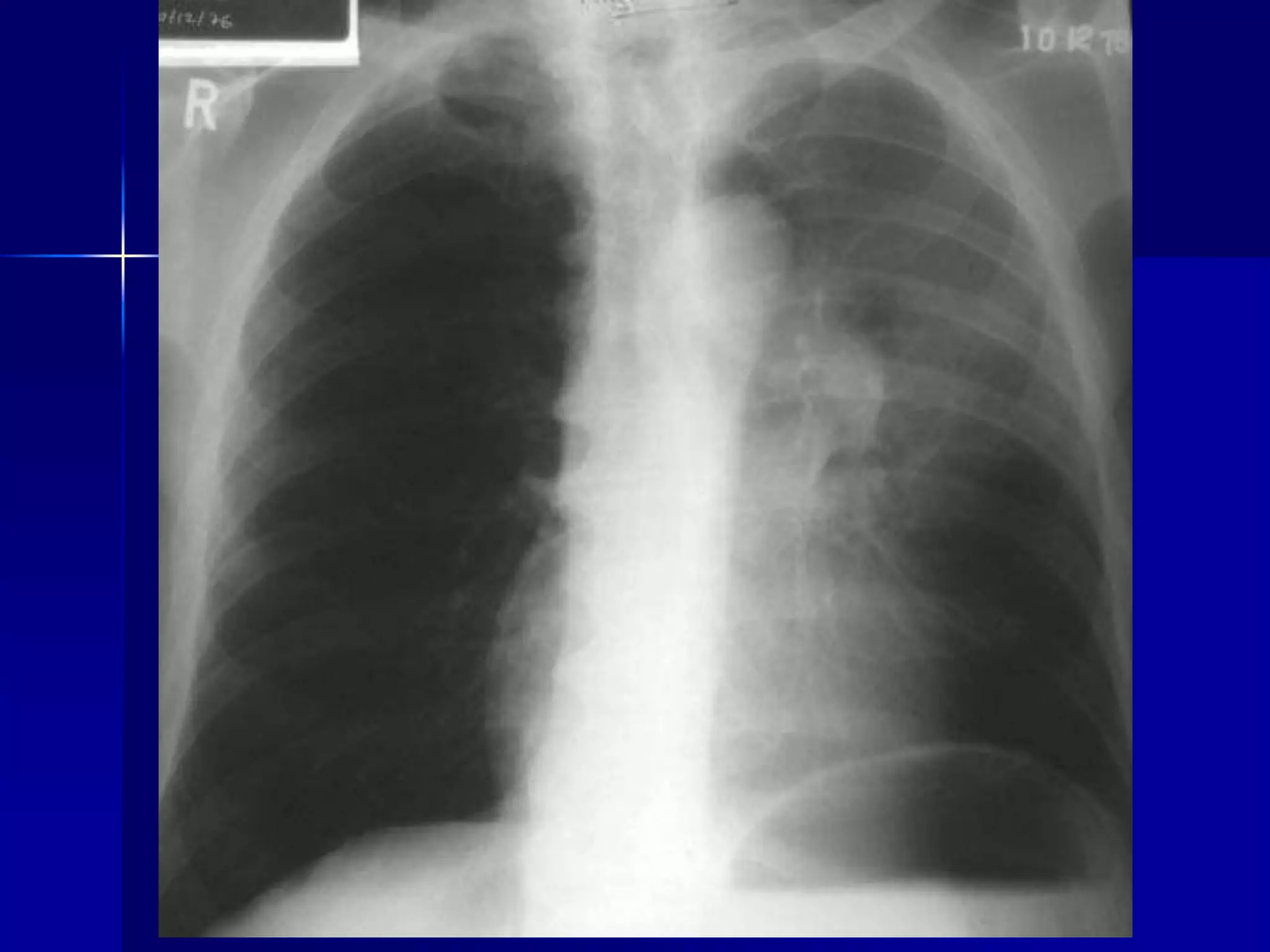
The document contains a review of various x-ray findings by Dr. Wedad Bardisi. It describes findings for different lung conditions including atelectasis, consolidation, pneumonia, and cancer. It also discusses other findings such as pleural effusions, cardiomegaly, bone metastases, fractures, and joint conditions like gout and rheumatoid arthritis. For each finding, it lists the key radiographic features that help in diagnosis.