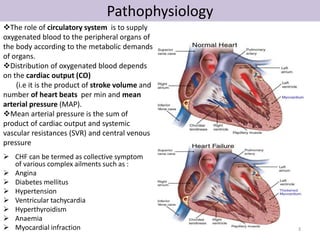
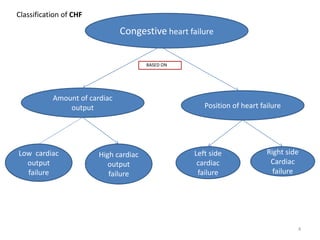
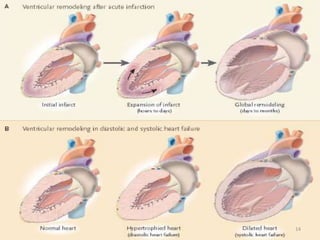
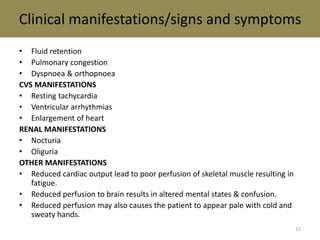
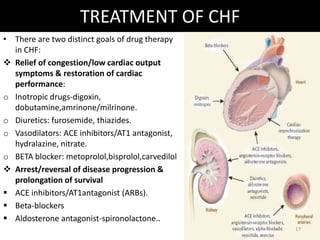
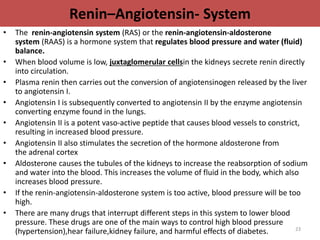
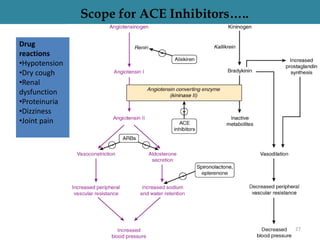
Congestive heart failure is a complex clinical syndrome characterized by abnormalities of left ventricular function and neurohormonal regulation. It occurs when the heart cannot pump enough blood to meet the body's needs. The pathophysiology involves compensatory mechanisms like increased sympathetic discharge and activation of the renin-angiotensin-aldosterone system which initially help but eventually worsen the heart's function. Congestive heart failure can be classified based on cardiac output level and the side of heart involved. Treatment focuses on relieving symptoms through diuretics, vasodilators, and other drugs while also arresting disease progression with ACE inhibitors, beta-blockers, and aldosterone antagonists.

![Potassium-Sparing Diuretics
• The K-sparing diuretics are weak diuretics alone.
• They are primarily used as adjuncts to thiazides and loop diuretics or for potassium and
magnesium spacing. Instead of using thiazides alone for hypertension ,triamterene is also
used by combination.
• Amiloride can be used for magnesium deficiency because it increases renal reabsorption.
• If a patient who has hypomagnesemia, and you can't give them enough magnesium
orally, because of laxative action, give amiloride.
• Also, amiloride is useful for patients taking lithium who have polyuria and complain of
having to get up three or four times at night. At a dose of 5 mg bid, amiloride reduces
urine volume by 30%.
• "Don't use any K-sparing diuretics with angiotensin-converting enzyme
inhibitors, angiotensin II receptor blockers [or] nonsteroidals.
• Be cautioned against using them when serum creatinine levels are above 2 mg/dL.
Specific side effects seen with K-sparing diuretics include
• Hyperchloremic acidosis;
• Hyperkalemia, especially if administered with an ACE inhibitor, angiotensin II receptor
blocker or in patients with diabetes;
• Gynecomastia, impotence in men or irregular menstrual cycles in women (only with use
of spironolactone);
• Folic acid deficiency (with chronic use of triamterene); or acute renal failure (with
triamterene when used with indomethacin [Indocin]).
21](https://image.slidesharecdn.com/chfbys-141030155903-conversion-gate02/85/CONGESTIVE-HEART-FAILURE-21-320.jpg)
![References
• Essential of Medical Pharmacology -K.D TRIPATHI.(P.GO 502-507)
• RANG & DALE’S Pharmacology (H.P RANG ,M.M DALE,J.M.RITTER,R.J.FLOWER .)PG.NO252-261.
• https://en.wikipedia.org/wiki/Renin-angiotensin_system
• CMDT 2007
• ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult:
Executive Summary.
http://group14.pbworks.com/w/page/16025091/DIURETICS
• "Diuretics." Drug Digest. June-July 2006. Express Scripts. 17 Nov. 2006
<http://www.drugdigest.org/DD/Comparison/NewComparison/0,10621,33-17,00.html#>.
• "Pharmacology of Diuretic Drugs." 17 Nov. 2006 <http://www.pharmacology.med.umn.edu/LEE-PHCL5103/
04DiureticNotes.pdf>.
http://www.cmellc.com/geriatrictimes/g010327.html
• Mende CW (1990), Current issues in diuretic therapy. Hosp Pract (Off Ed) 25(suppl 1):15-21 [see
discussion pp30-31].
44](https://image.slidesharecdn.com/chfbys-141030155903-conversion-gate02/85/CONGESTIVE-HEART-FAILURE-44-320.jpg)










































































