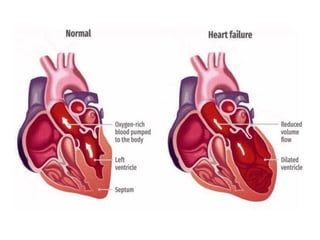
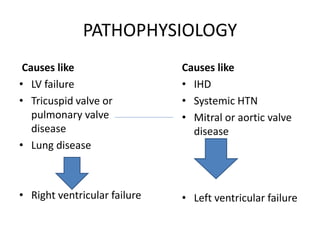
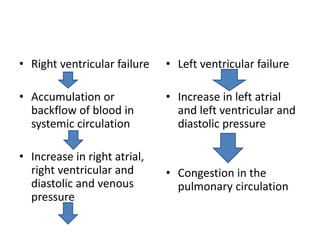
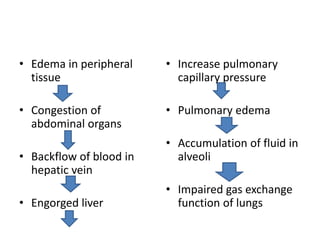
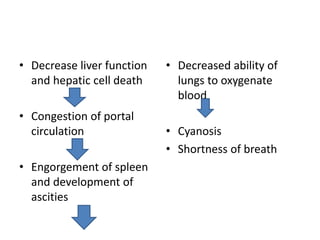
Congestive heart failure (CHF) is a syndrome characterized by the heart's inability to pump sufficient blood to meet the body's needs, resulting in impaired cardiac output and congestion. It can be classified into left-sided and right-sided failure, with left-sided failure being the most common form, leading to pulmonary congestion and edema, while right-sided failure causes systemic venous congestion. Diagnosis involves physical exams, lab tests, and imaging, with management including lifestyle modifications, pharmacological treatments, and potentially surgical interventions.
























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







