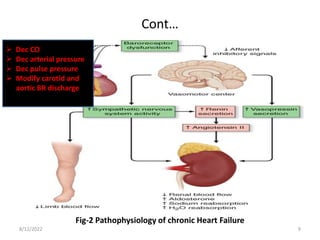
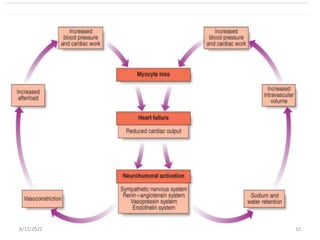
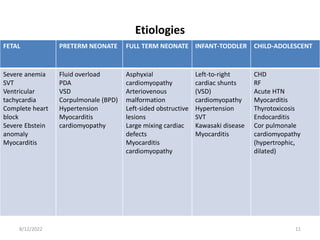
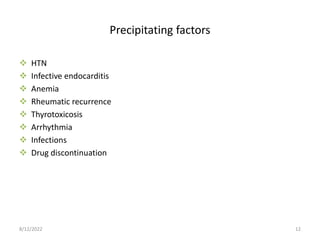
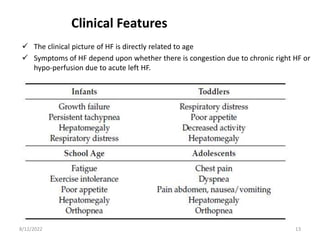
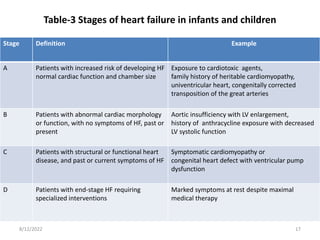
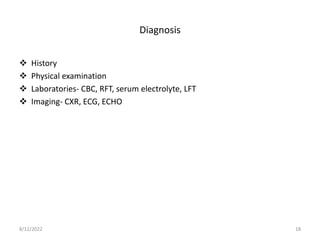
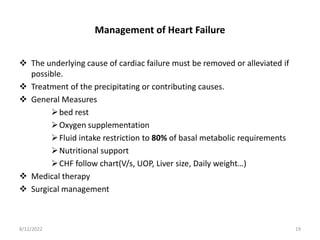
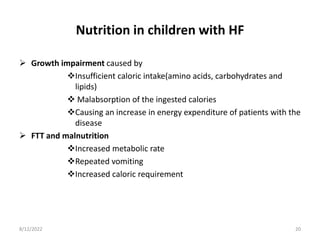
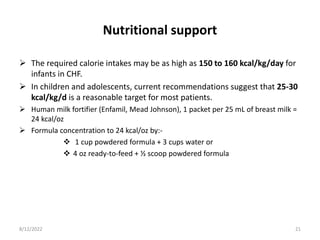
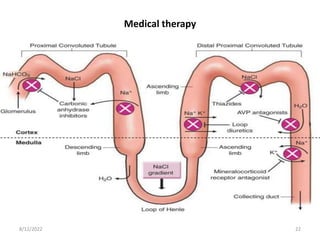
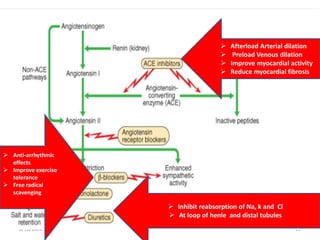
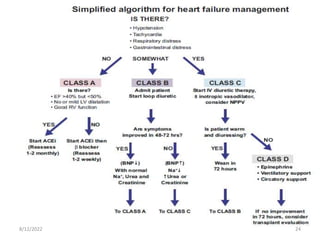
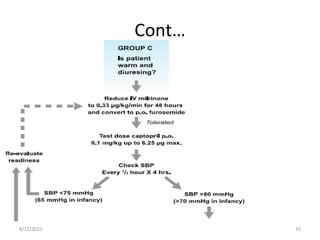
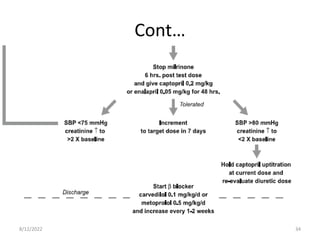
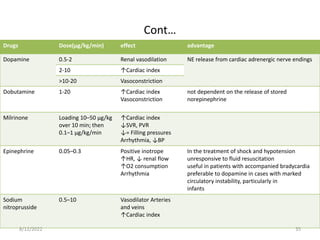
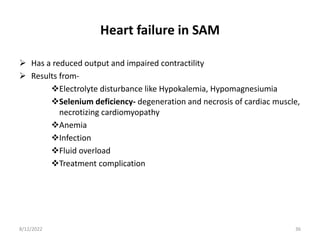
This document discusses congestive heart failure in children. It defines heart failure as the heart's inability to pump enough blood to meet the body's needs. The main causes are ventricular dysfunction from volume or pressure overload. Symptoms depend on whether there is right or left ventricular failure. Treatment involves addressing the underlying cause, managing precipitating factors, restricting fluids, using diuretics and other medications, and considering interventions like transplantation for refractory cases.


























![Acute heart failure [MBBS]](https://cdn.slidesharecdn.com/ss_thumbnails/acuteheartfailure-170323061012-thumbnail.jpg?width=640&height=640&fit=bounds)




















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


