Downloaded 90 times
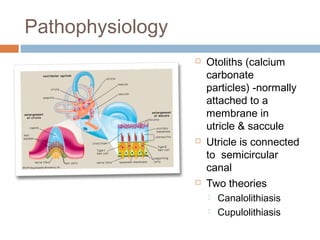

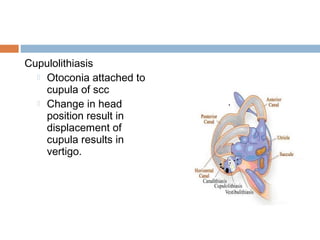























Benign paroxysmal positional vertigo (BPPV) is the most common cause of positional vertigo. It involves abnormal sensations of movement triggered by certain head positions. Calcium particles in the inner ear can become dislodged and enter the semicircular canals, stimulating hair cells and causing vertigo. The Dix-Hallpike maneuver is used for diagnosis - a patient is positioned to provoke nystagmus if BPPV is present. Treatment involves maneuvers like the Epley maneuver to reposition the particles.















































































