Downloaded 136 times
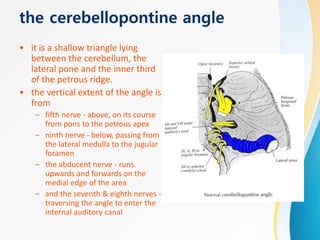























The cerebellopontine angle is a triangular area located between the cerebellum, pons, and petrous ridge. It contains several cranial nerves including the 5th, 7th, and 8th nerves. Lesions in this area often damage the 7th and 8th nerves, causing symptoms like hearing loss, tinnitus, and facial weakness. A clinical exam assessing the function of these nerves can help localize pathologies in the cerebellopontine angle.










































![Facial nerve and its applied aspect - seminar 3 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facialnerveanditsappliedaspect-seminar3autosaved-231021155352-8463bc10-thumbnail.jpg?width=640&height=640&fit=bounds)












































