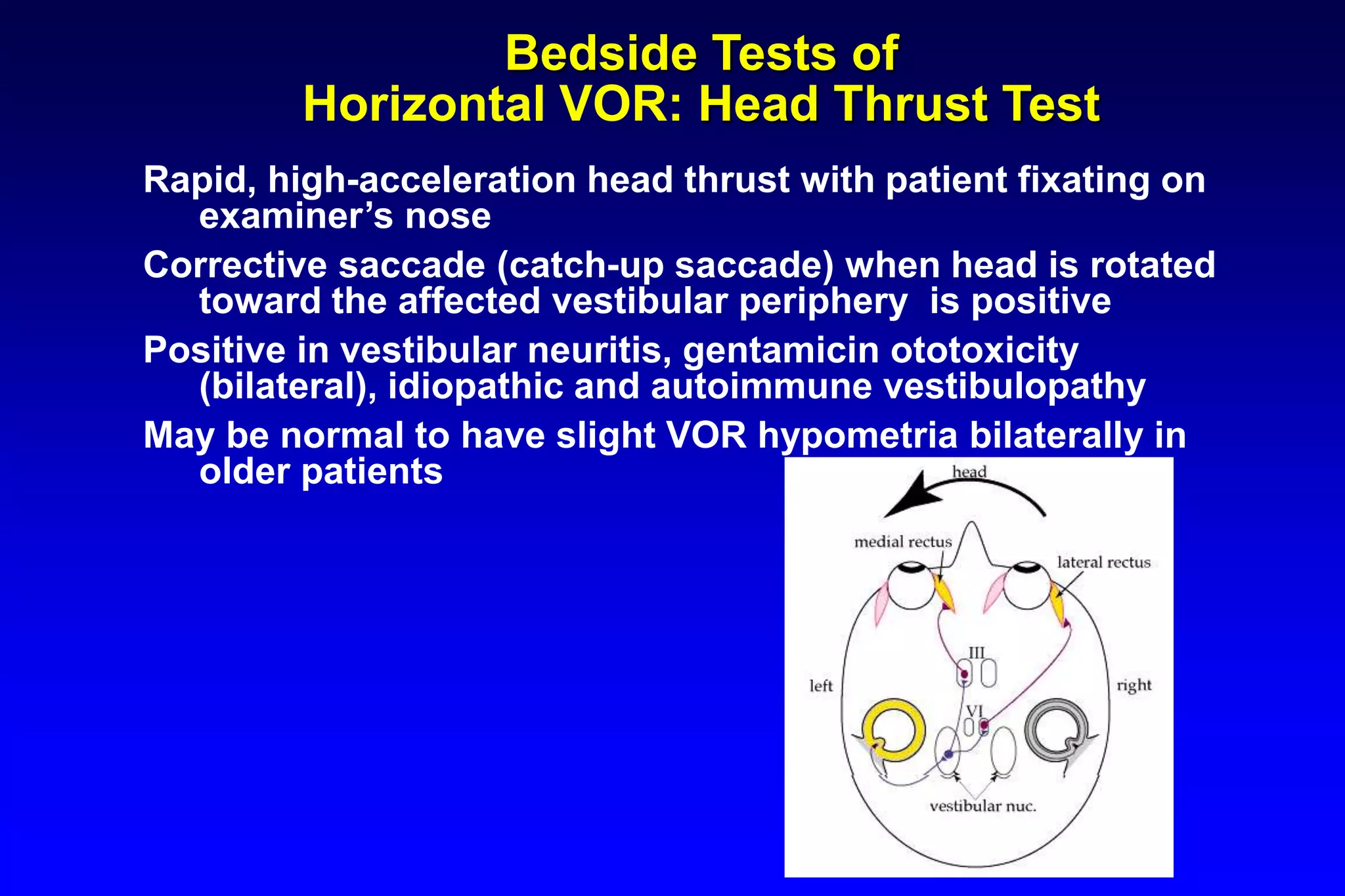
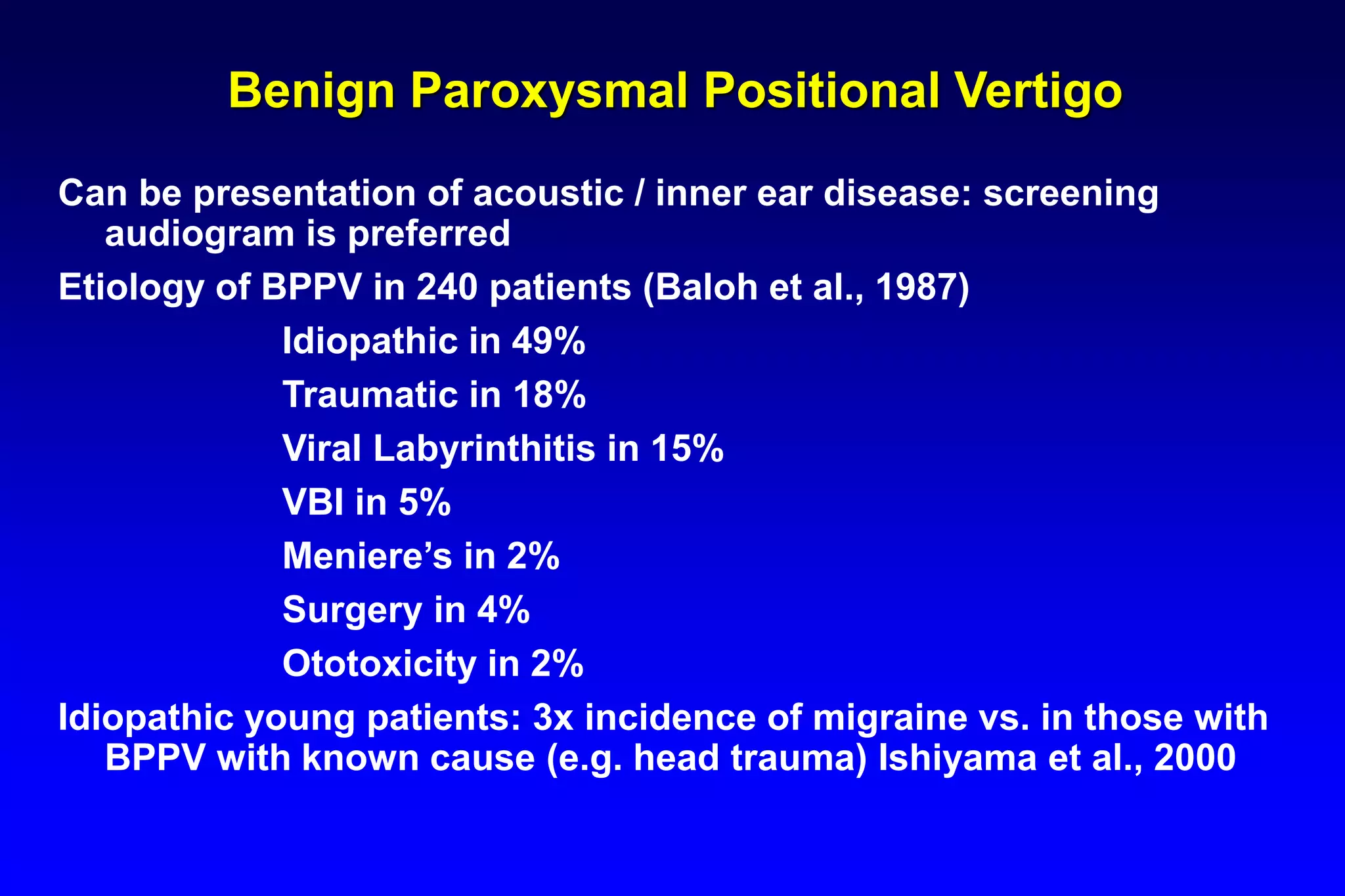
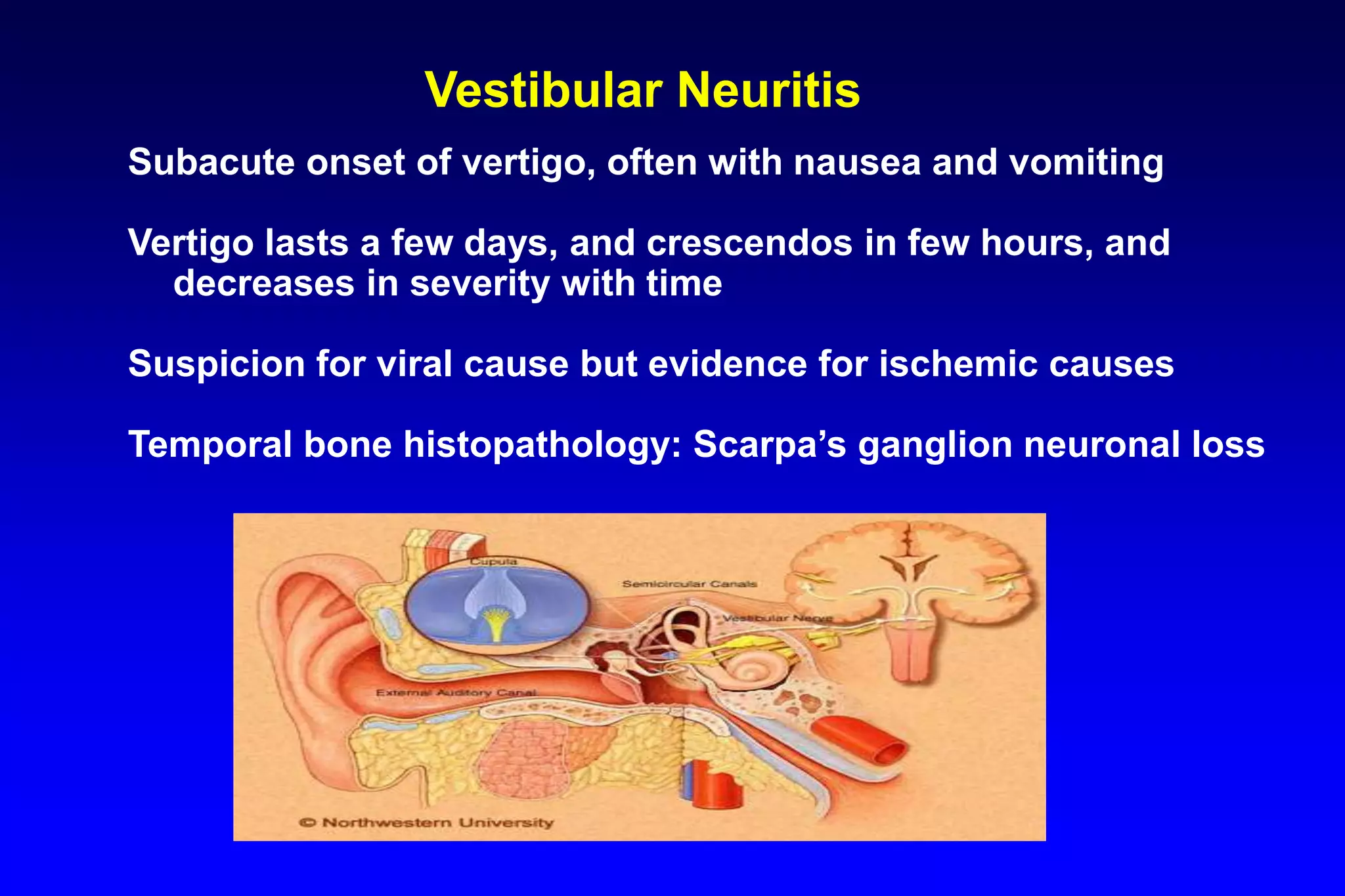
This document discusses dizziness and vertigo from an otoneurological perspective. It begins by outlining key questions to ask patients regarding the nature and characteristics of their dizziness. It then describes potential otologic and neurological symptoms. Specific balance and vestibular tests are discussed, including nystagmus patterns, bedside tests like head thrust and positional maneuvers for BPPV. Common causes of vertigo like BPPV, vestibular neuritis, Meniere's disease, migraines, and strokes are explained. Appropriate use of anti-vertigo medications is emphasized.