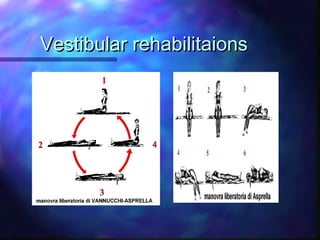
Benign paroxysmal positional vertigo (BPPV) is caused by loose particles in the inner ear that disrupt balance. It is one of the most common causes of vertigo. Canalith repositioning procedures (CRPs) like the Epley maneuver are first-line treatments that are effective at resolving BPPV symptoms in over 75% of patients by repositioning the particles. While usually benign and self-limiting, BPPV can recur in about 13% of cases within 6 months if not treated with CRPs or vestibular rehabilitation exercises.