Downloaded 51 times



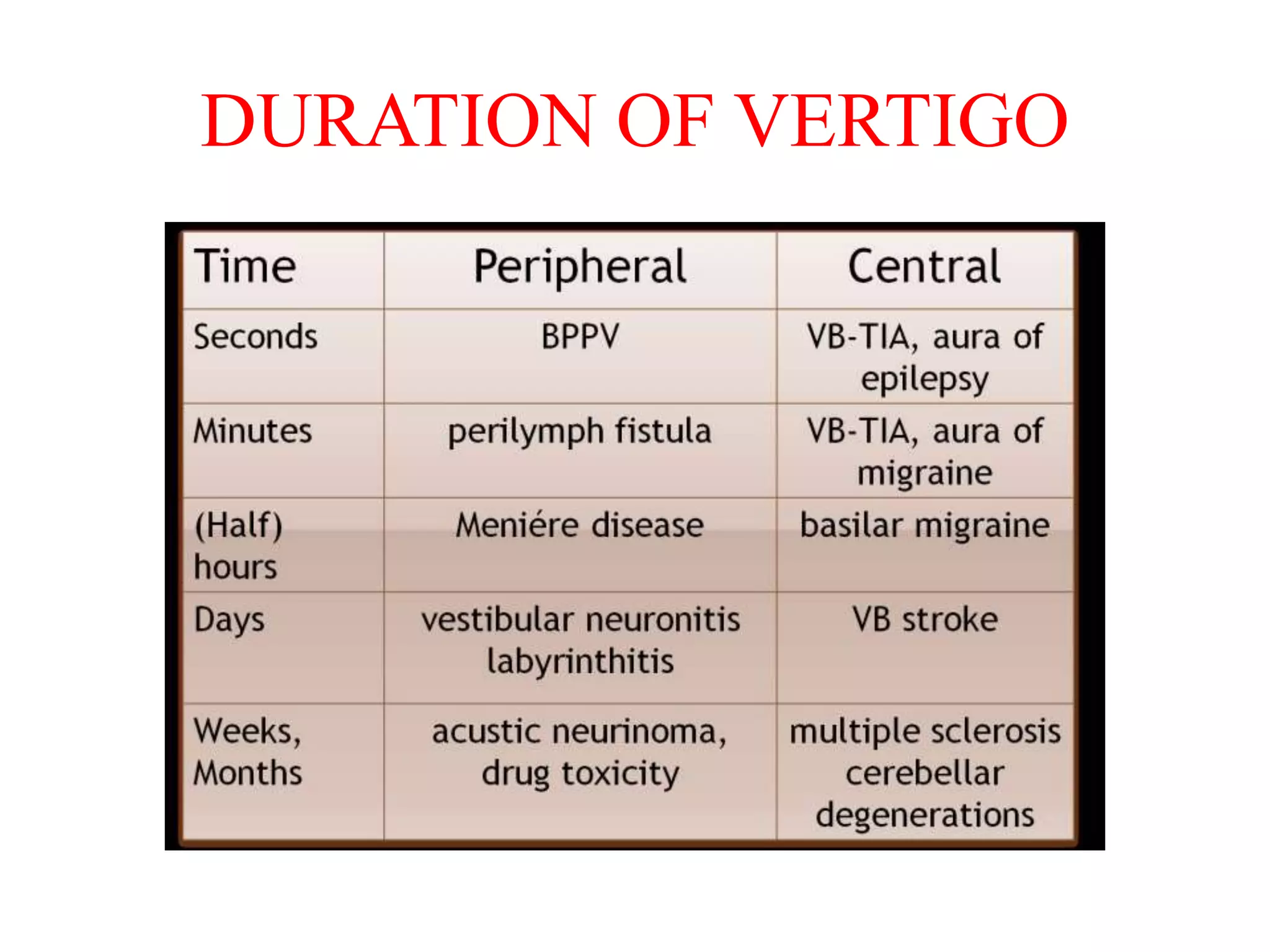















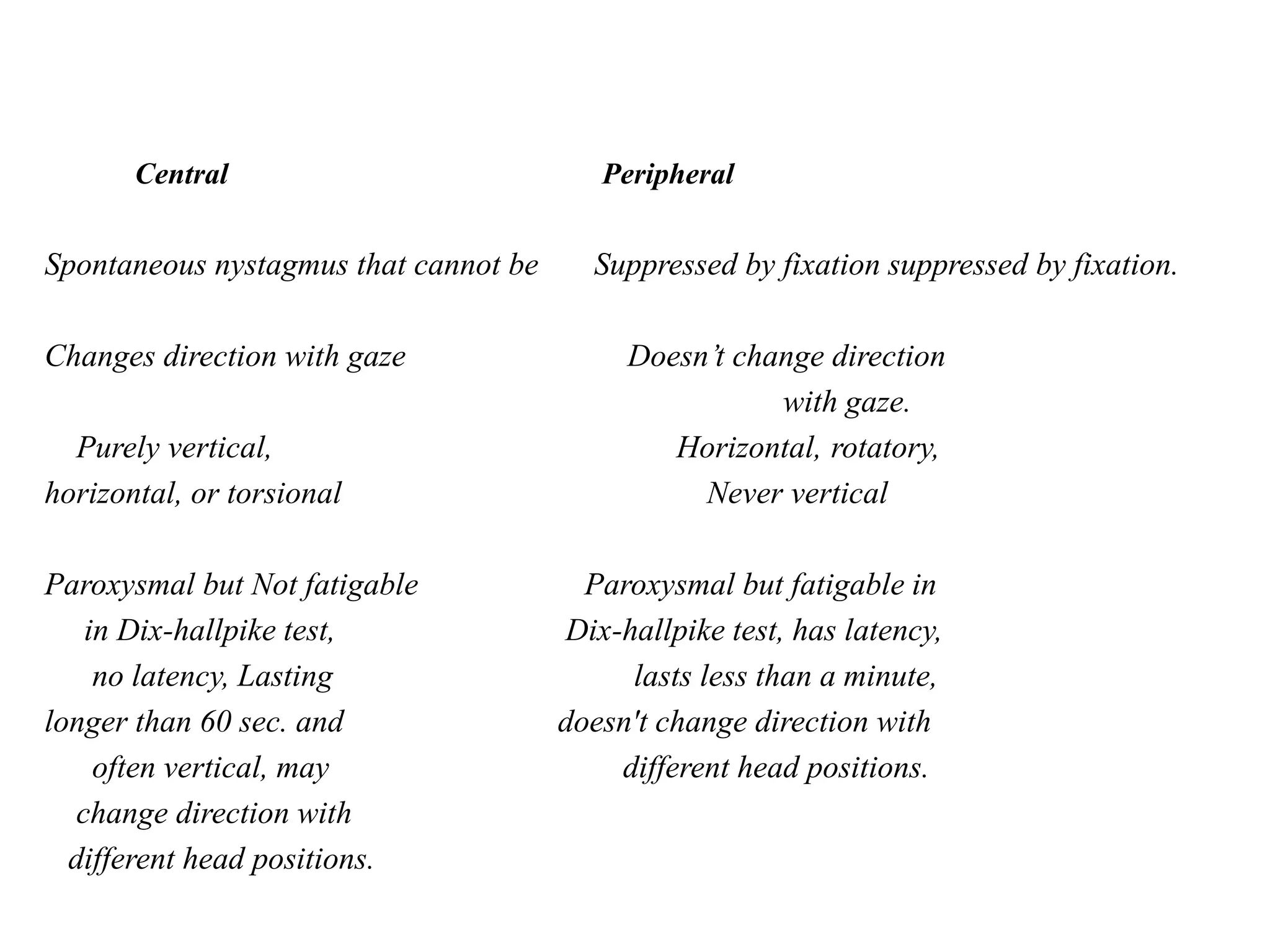














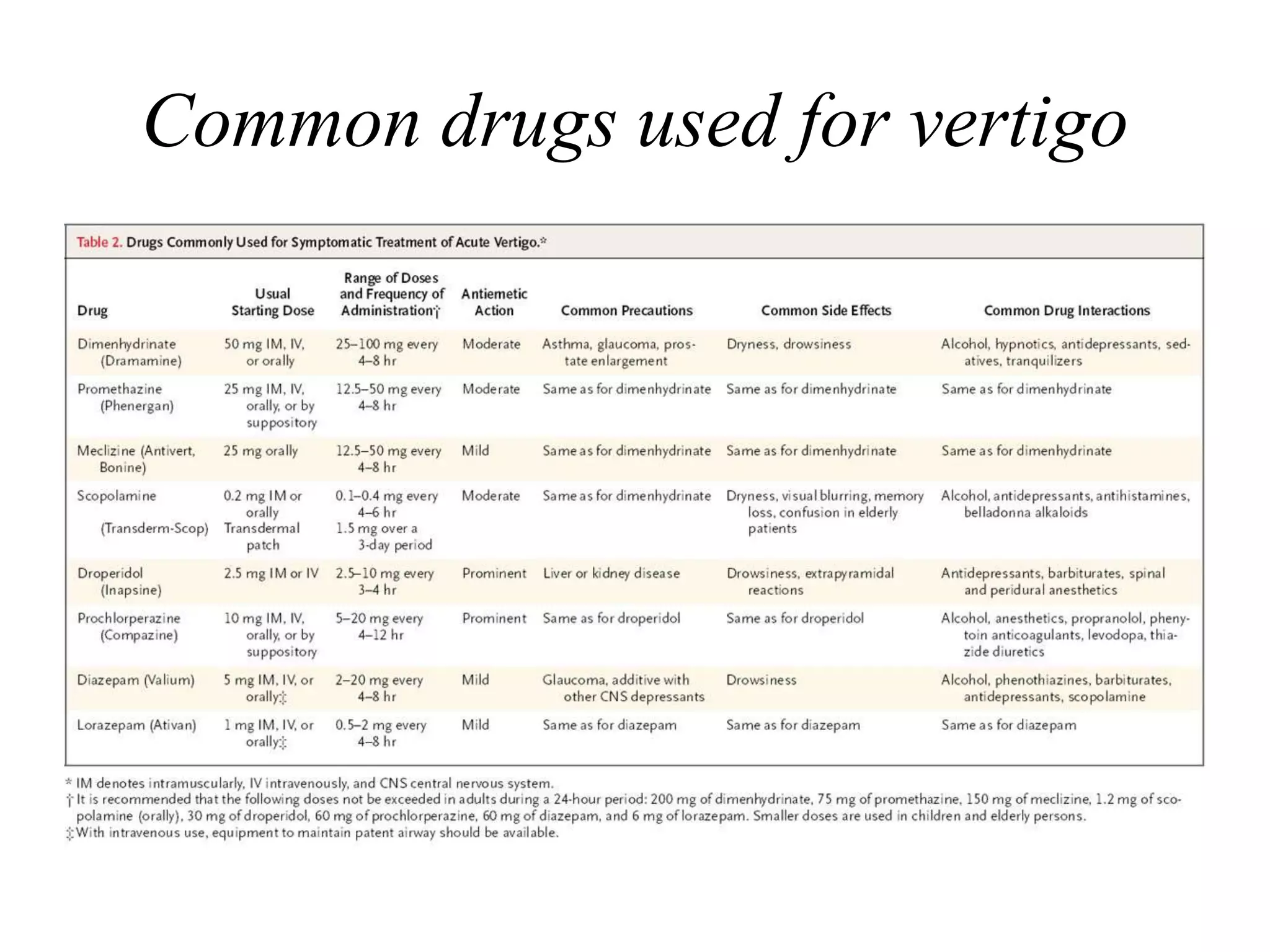

















This document discusses vertigo, including its causes and management. It defines vertigo as a subjective sense of imbalance or spinning. The vestibular system, which includes the inner ear and brainstem regions, provides input about movement and spatial orientation. Disruptions in the vestibular system or its central connections can cause vertigo. Common causes include benign paroxysmal positional vertigo (BPPV), Ménière's disease, vestibular neuronitis, and acoustic neuromas. Treatment depends on the cause but may include repositioning maneuvers, medications, or surgery. A thorough history and physical exam are important for diagnosis.























































































