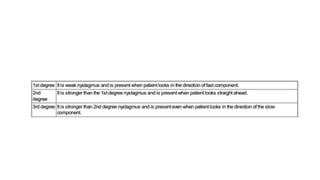
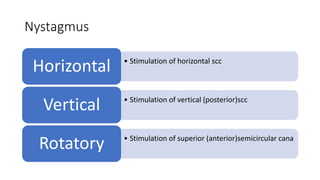
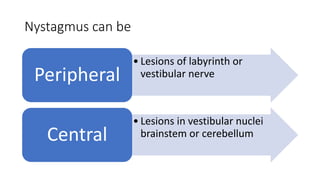

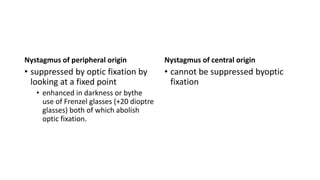
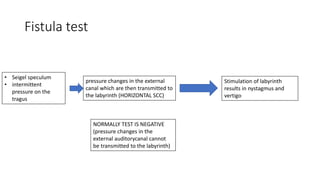
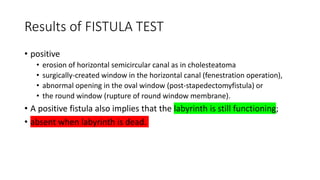
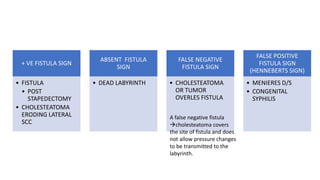
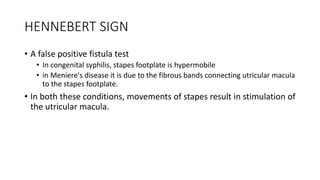

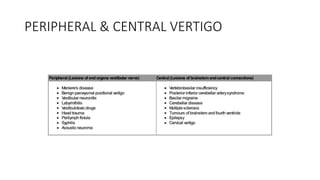
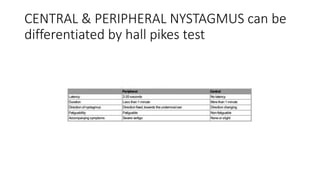

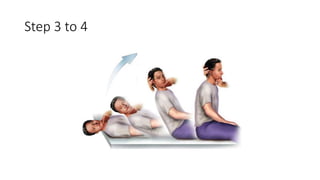

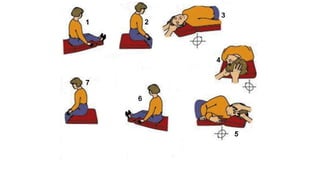
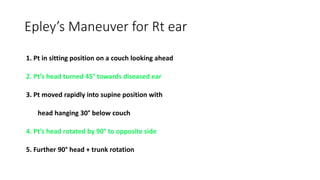



This document discusses tests used to assess vestibular function, including nystagmus, caloric testing, fistula testing, optokinetic testing, and galvanic testing. It also covers peripheral vestibular disorders like BPPV and vestibular neuronitis, as well as central causes of nystagmus. Diagnosis and treatment of BPPV is discussed, including Epley's maneuver and surgical options.























































































