












![Dix-Hallpike test [anterior or posterior canal
benign paroxysmal positional vertigo]
1. The patient sits on the bed or examination table, and the head is
turned
2. 45 degrees horizontally toward the labyrinth to be tested
(position 1).
3. The examiner quickly brings the head and trunk straight back
“en bloc,” so that the head is hanging over the edge of the
examination table by 20 to 30 degrees (position 2).
4. The examiner asks whether the patient has vertigo and observes
for nystagmus.
5. The patient’s upper body is then brought up slowly to a sitting
position with the head still turned 45 degrees, and nystagmus is
sought again.
6. This test then is repeated with the head turned 45 degrees in the
other direction.
NIHS, Kol:Mobility P&R,MDN:IAP-WB,2015](https://image.slidesharecdn.com/ap-bppv-iap2015-151105101056-lva1-app6892/75/BPPV-Physical-Diagnosis-and-Management-15-2048.jpg)

![Side-lying test [for anterior or posterior canal
benign paroxysmal positional vertigo]
1. The patient sits on the bed or examination table with the legs
over the side, and the head is rotated 45 degrees horizontally
away from the labyrinth to be tested (position 1).
2. The examiner then quickly brings the patient’s head and trunk
down on the side opposite to the direction the head is turned
(position 2).
3. The patient is asked to report any vertigo and is observed for
nystagmus.
4. The patient is then brought to a sitting position with the head still
turned 45 degrees, and the examiner rechecks for nystagmus and
vertigo.
5. The test is repeated with head turned 45 degrees horizontally to
the other side.
NIHS, Kol:Mobility P&R,MDN:IAP-WB,2015](https://image.slidesharecdn.com/ap-bppv-iap2015-151105101056-lva1-app6892/75/BPPV-Physical-Diagnosis-and-Management-17-2048.jpg)

![Roll test [for horizontal canal benign paroxysmal
positional vertigo]
1. The patient is laid supine with the head flexed 20 degrees.
2. The head is quickly rolled to one side, nystagmus is looked
for and the patient is asked to report any vertigo.
3. The head is then slowly rolled back to a supine position.
4. The head is then quickly rolled to the other side,
nystagmus is looked for, and the patient is asked to report
any vertigo. (Modified from Tusa and Herdman, 1998.4)
NIHS, Kol:Mobility P&R,MDN:IAP-WB,2015](https://image.slidesharecdn.com/ap-bppv-iap2015-151105101056-lva1-app6892/75/BPPV-Physical-Diagnosis-and-Management-19-2048.jpg)
![Test Series [vertigo when lying on the right
side]
The series is as follows:
1. Perform the Dix-Hallpike test on the left side.
2. Perform the Dix-Hallpike test on the right side.
3. If the patient has no vertigo: Before sitting the patient
up from the right side, perform a roll test by having the
patient turn the head quickly to the left.
4. After 30 seconds, have the patient quickly turn the
head back to the right.
5. After 30 seconds, have the patient sit up.
NIHS, Kol:Mobility P&R,MDN:IAP-WB,2015](https://image.slidesharecdn.com/ap-bppv-iap2015-151105101056-lva1-app6892/75/BPPV-Physical-Diagnosis-and-Management-20-2048.jpg)








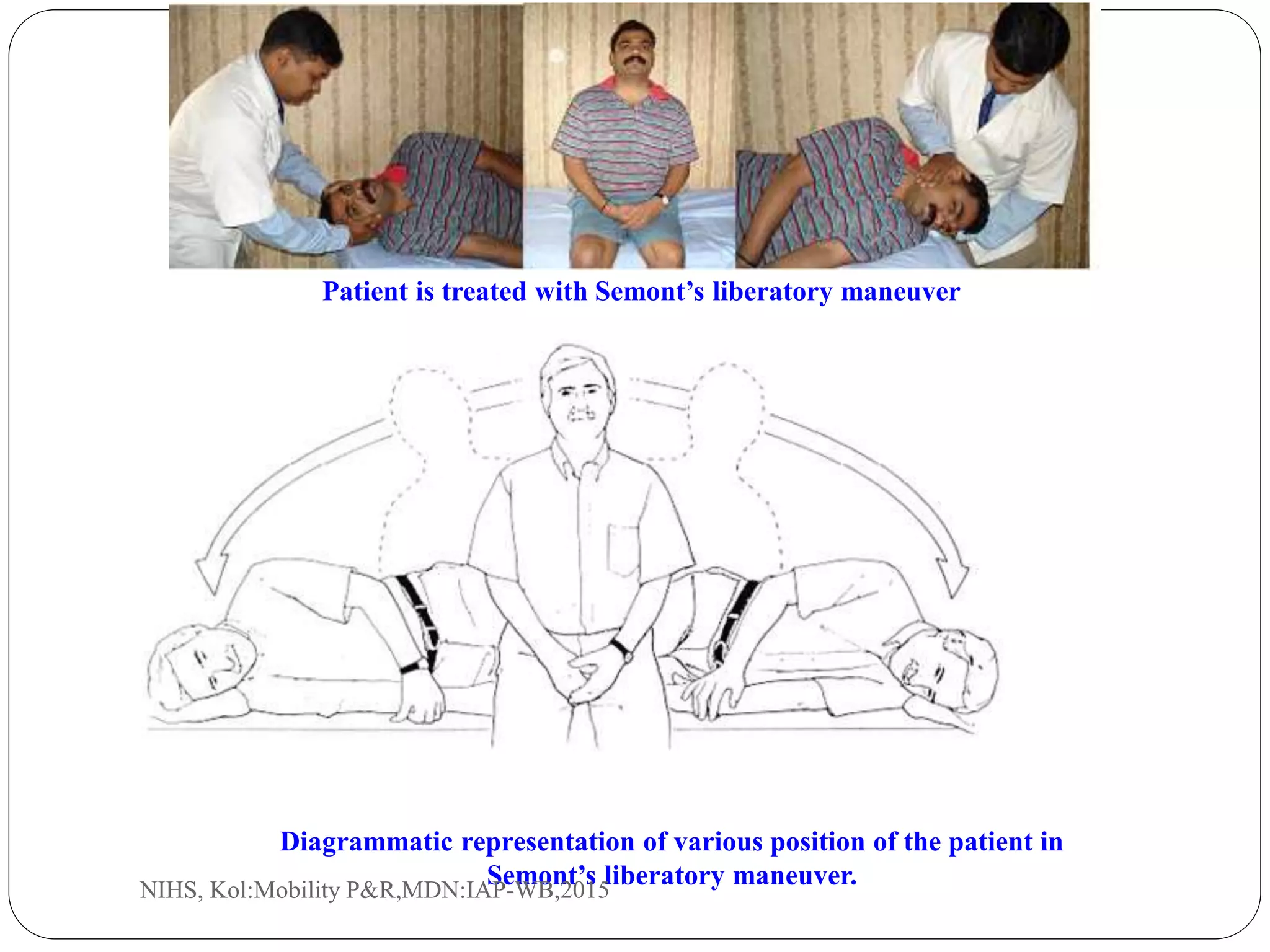



![Brandt-Daroff treatment [for treatment of
posterior semicircular canal benign paroxysmal positional vertigo]
The patient is moved quickly into the side-lying
position on the affected side and stays in that position
until 30 seconds after the vertigo has stopped.
The patient then sits up and again waits for the vertigo
to stop. The patient then repeats the movement to the
opposite side, stays there for 30 seconds after vertigo
stops, and sits up.
The entire treatment is repeated 10 to 20 times, three
times a day, until the patient has no vertigo for 2 days
in a row. AC anterior canal; PC posterior canal. Black
arrows indicate position and movement of debris.
(Modified from Tusa and Herdman, 1998.4)
NIHS, Kol:Mobility P&R,MDN:IAP-WB,2015](https://image.slidesharecdn.com/ap-bppv-iap2015-151105101056-lva1-app6892/75/BPPV-Physical-Diagnosis-and-Management-33-2048.jpg)











The document discusses Benign Paroxysmal Positional Vertigo (BPPV), a common cause of vertigo, characterized by brief episodes of dizziness triggered by specific head movements. BPPV results from debris in the inner ear, leading to abnormal signals sent to the nervous system, and can be diagnosed using tests like the Dix-Hallpike maneuver. Treatment options include various repositioning maneuvers, such as the Epley and Semont maneuvers, to dislodge the debris and alleviate symptoms.



































































































