Downloaded 17 times

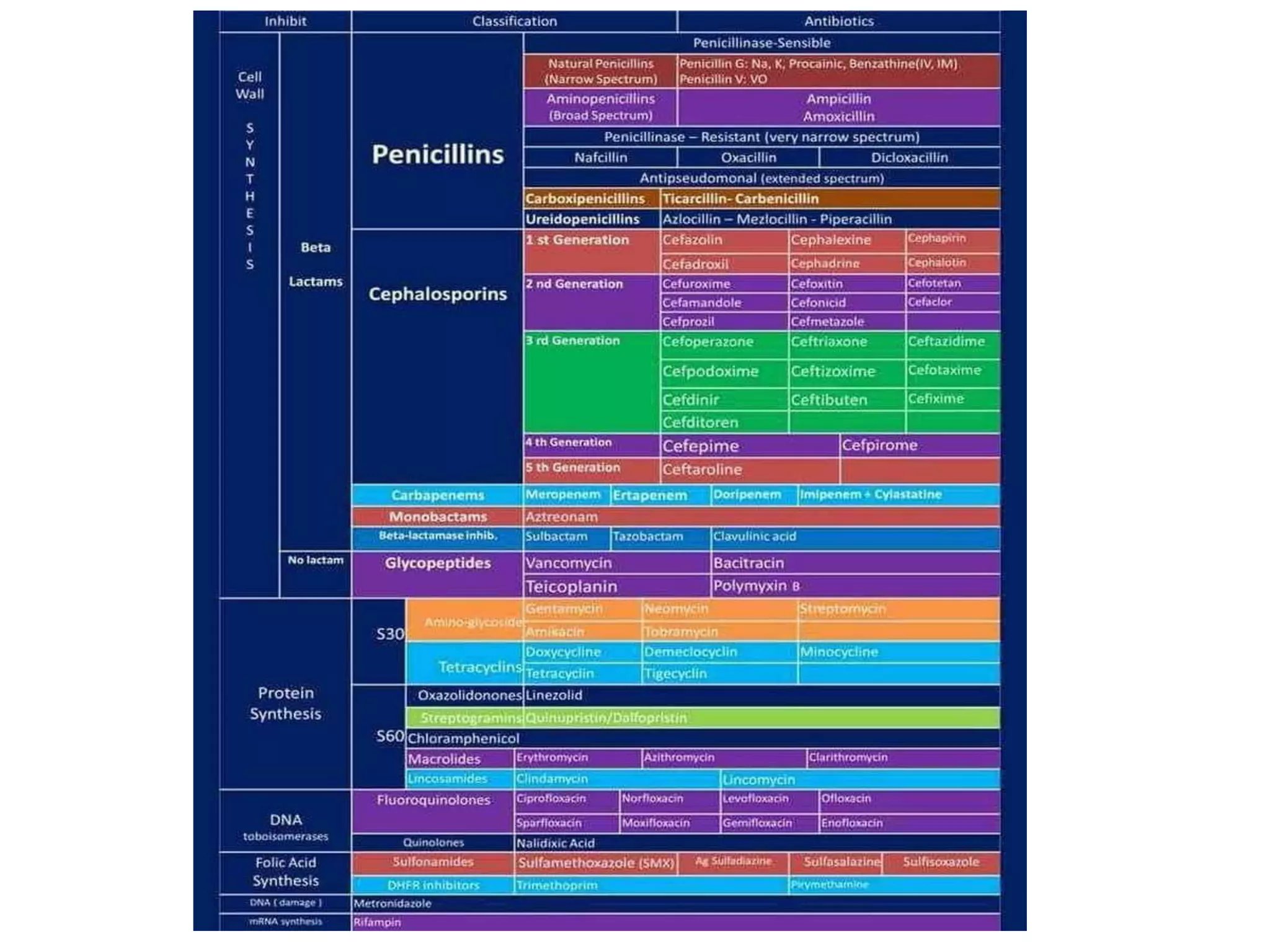


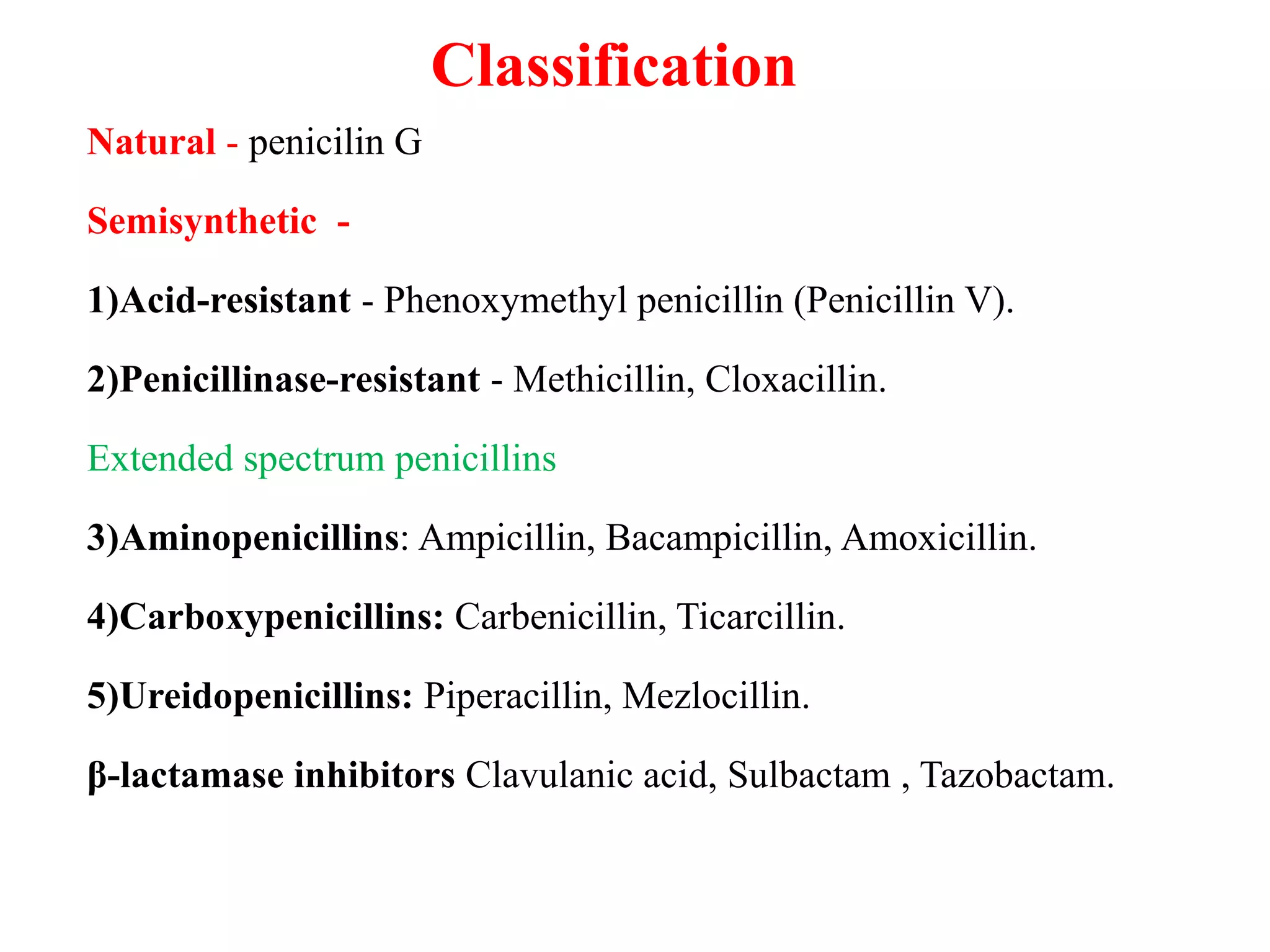













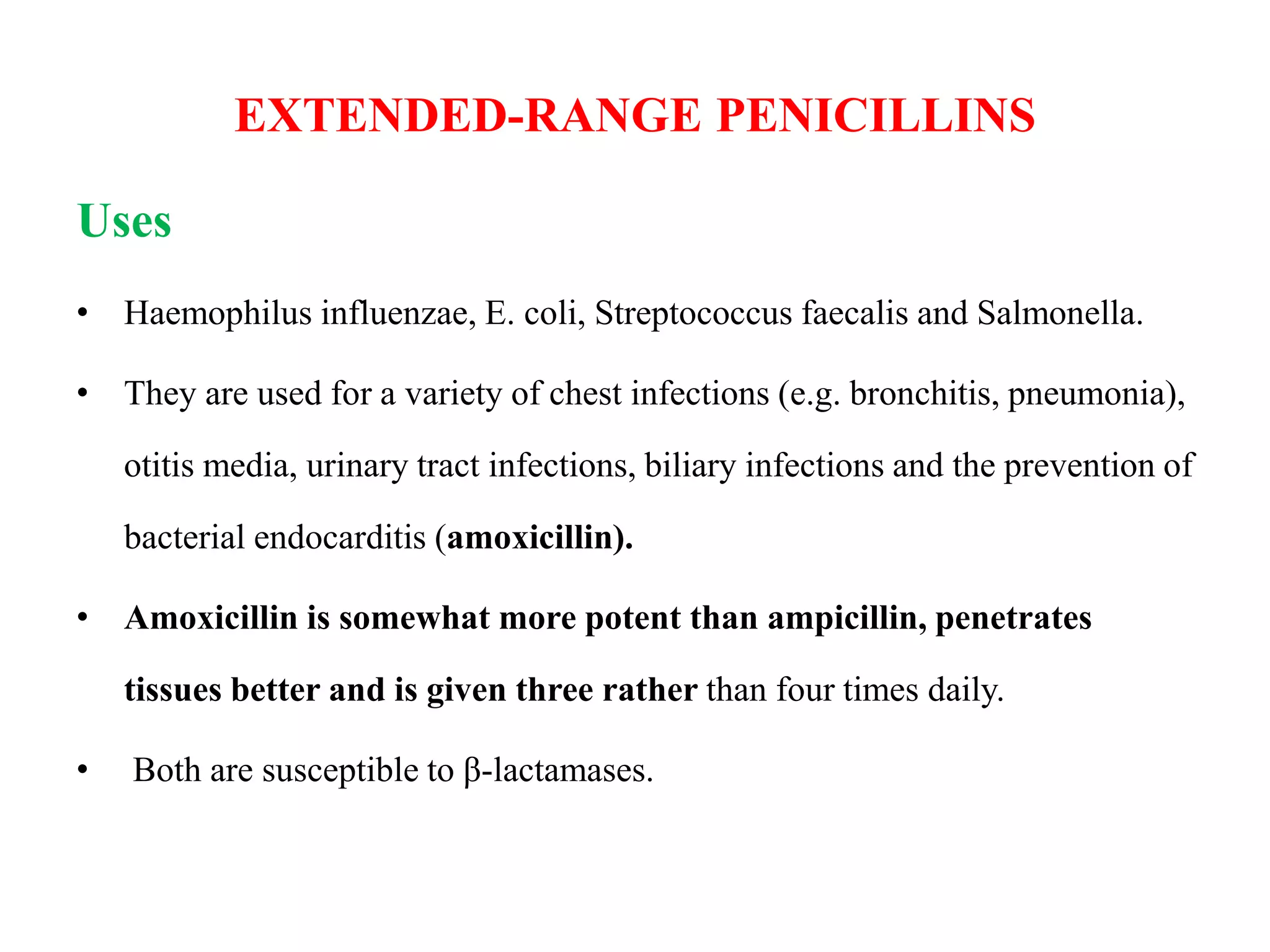









The document provides an overview of beta-lactam antibiotics, focusing on penicillins, including their history, classification, mechanisms of action, uses, resistance, and adverse effects. It details various types of penicillins, their pharmacokinetics, and specific indications for use in bacterial infections, especially in medical and dental practices. Additionally, the document highlights the limitations and precautions related to penicillin usage, including hypersensitivity reactions and the development of resistance.


































































![Tools of dental_public_health[1]](https://cdn.slidesharecdn.com/ss_thumbnails/toolsofdentalpublichealth1-151108134342-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)



















