











![IMIDAZOLES AND TRIAZOLES
● Azoles are predominantly fungistatic.
● They inhibit C-14 α-demethylase (a cytochrome P450 [CYP450]
enzyme),
● This blocks the demethylation of lanosterol to ergosterol, the principal
sterol of fungal membranes
● The inhibition of ergosterol biosynthesis disrupts membrane structure and
function, which, in turn, inhibits fungal cell growth.
Jegan](https://image.slidesharecdn.com/antifungal-200413184507/75/Antifungal-Drugs-25-2048.jpg)










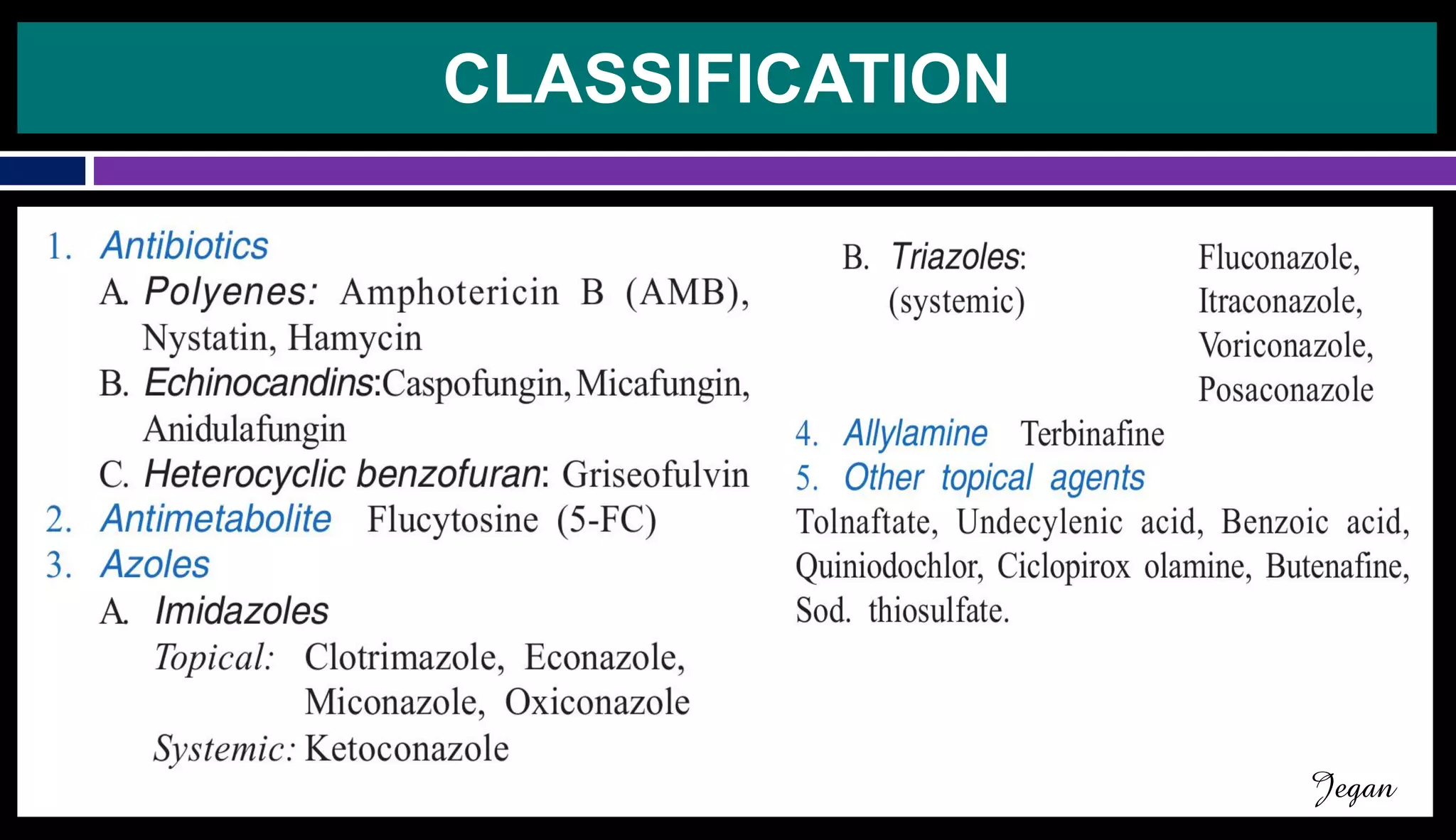
The document provides an overview of antifungal drugs, detailing their mechanisms of action, classifications, and specific examples such as amphotericin B, echinocandins, azoles, and allylamines. It highlights the structural differences between fungi and bacteria that make targeting fungal infections unique, as well as the therapeutic applications and potential adverse effects of various antifungal agents. Key points include the effectiveness of different drug classes against specific fungal infections and their respective pharmacokinetics.
Overview of antifungal drugs, mycoses, characteristics of fungi, and implications for treatment.
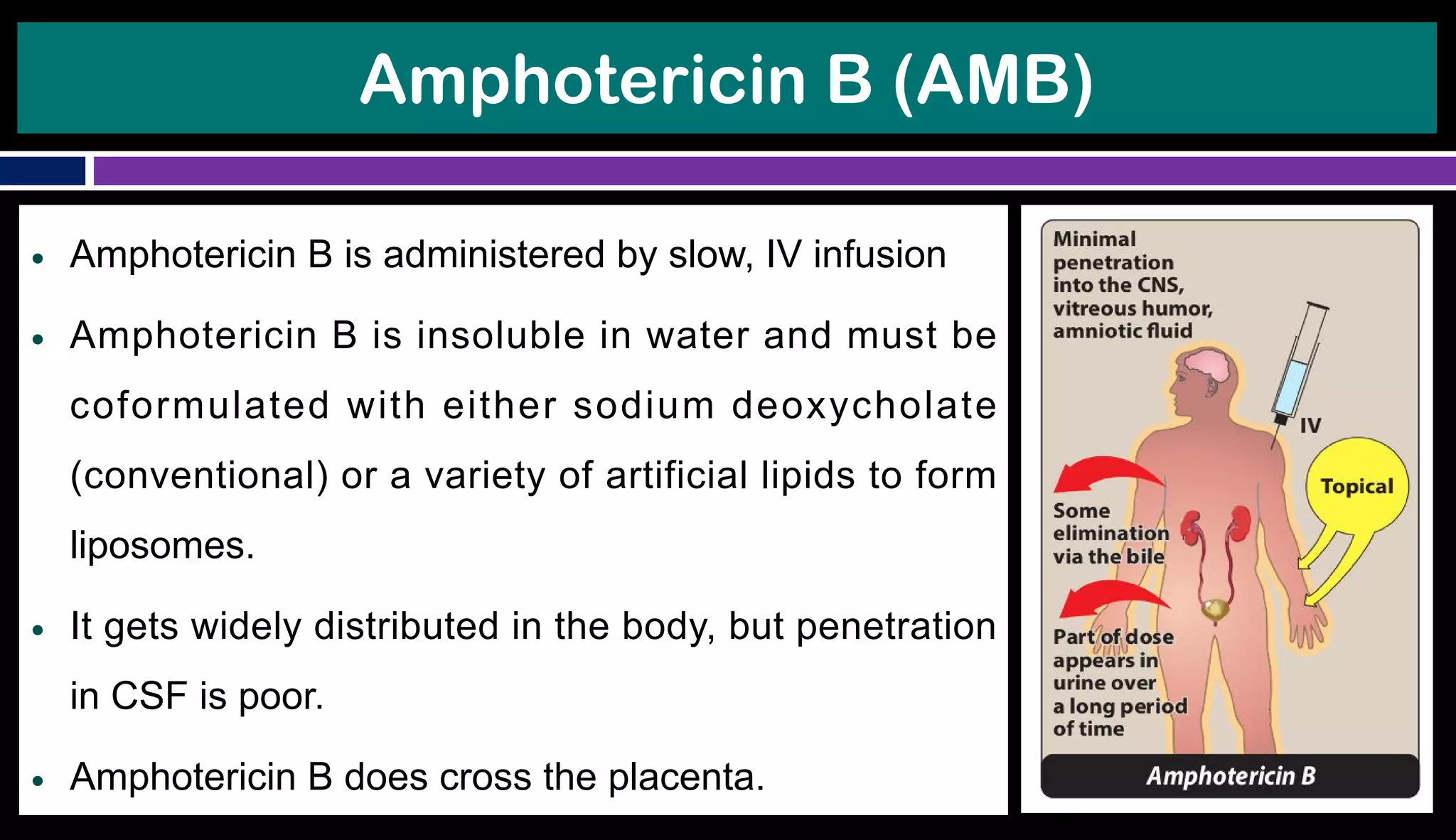
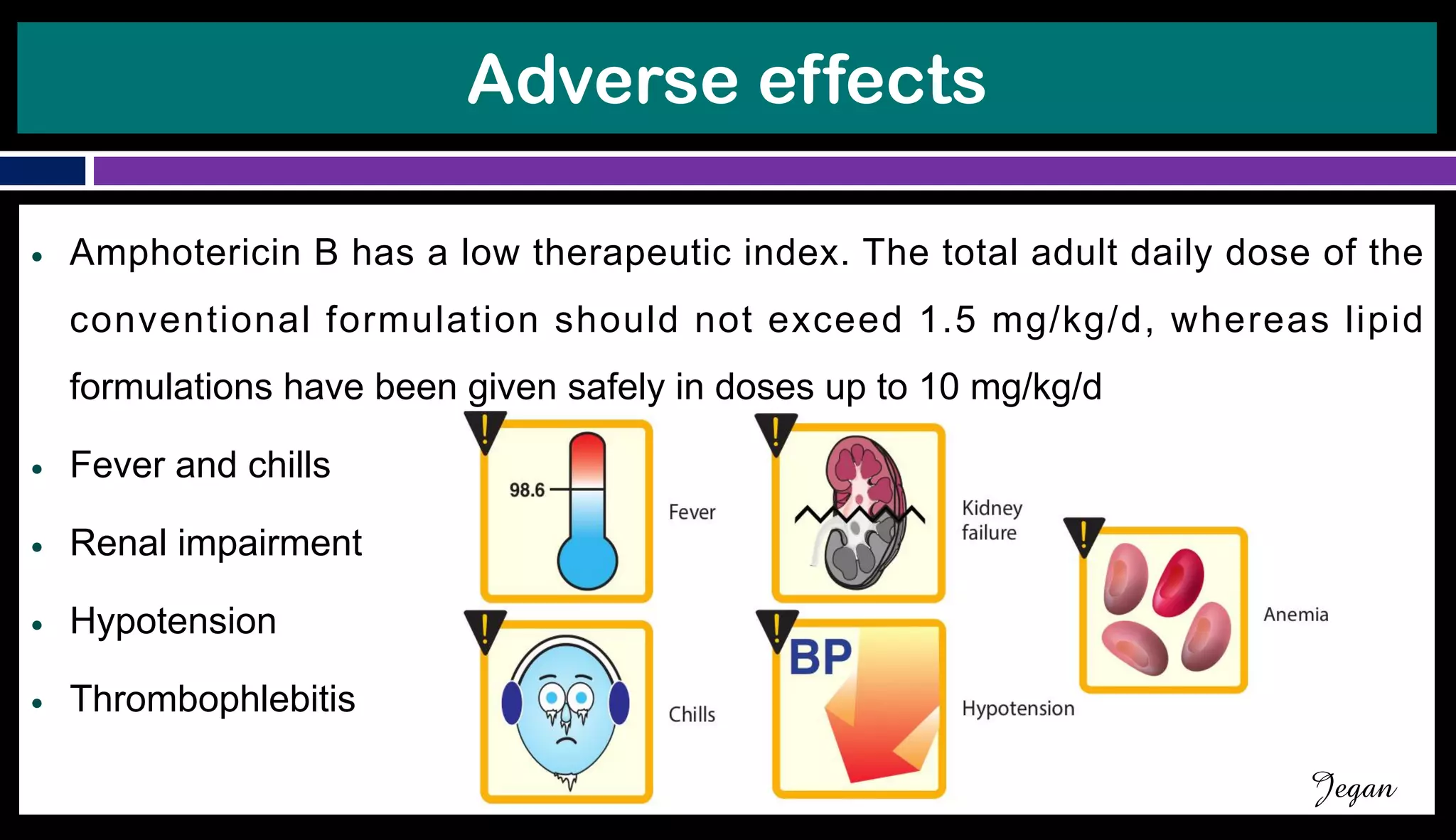
Focus on Amphotericin B, its mechanism of action, administration details, and adverse effects.
Introduction to Echinocandins with a focus on Caspofungin, its unique mechanism, and effects.
Discussion on Griseofulvin, its uses, absorption challenges, and interactions.
Description of Flucytosine, its mechanism of action, efficacy, toxicity, and absorption properties.
Classification of azole antifungals, their mechanisms, and specific drugs like Clotrimazole and Ketoconazole.
Description of Terbinafine, its action mechanism, and effects on fungal cell membranes.
Thank you note, concluding the presentation.























































































