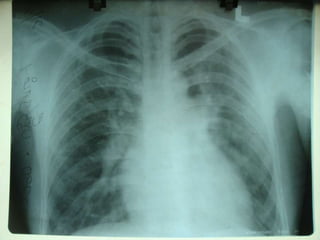
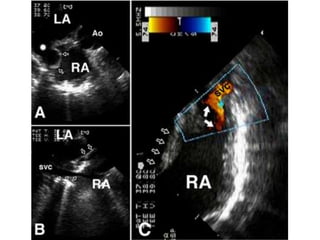
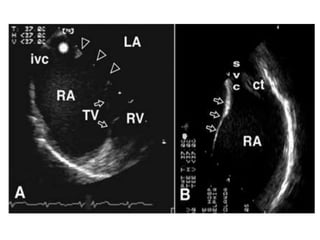
- The patient is a 36-year-old male who presented with palpitations and breathlessness on exertion. Echocardiogram revealed an atrial septal defect (ASD) of the sinus venosus type with anomalous pulmonary venous drainage and moderate pulmonary hypertension.
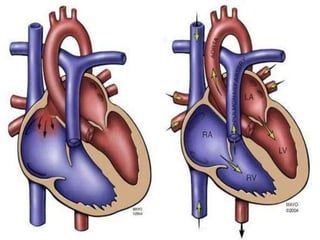
- Sinus venosus ASDs account for 10% of ASDs and involve a defect between the superior vena cava and right atrium, often associated with anomalous pulmonary vein drainage.
- Surgical repair is the treatment of choice, involving use of a patch to redirect pulmonary vein flow to the left atrium while closing the interatrial communication.