Downloaded 93 times
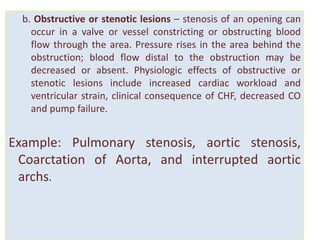
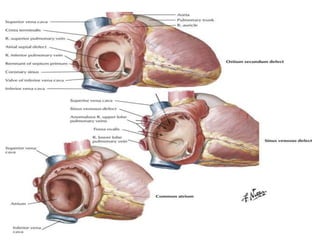
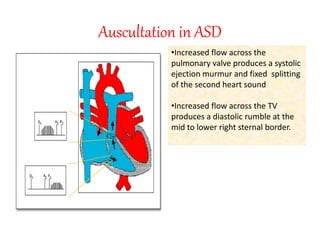
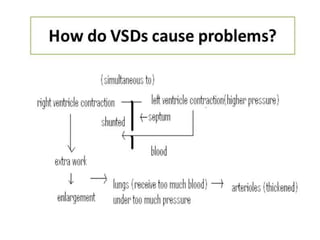
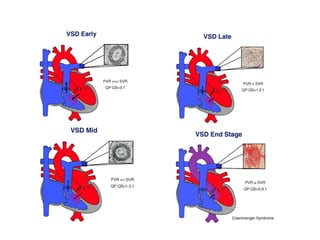
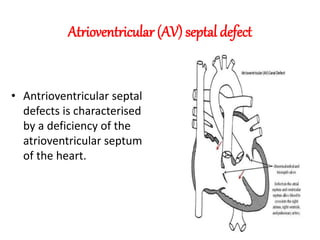
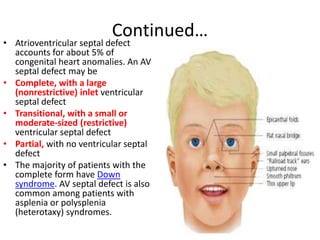
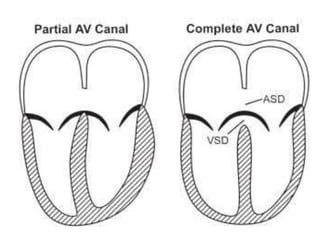
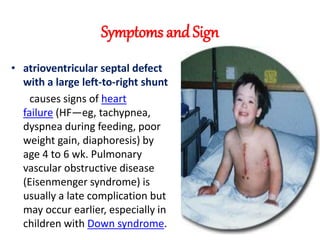


The document discusses acyanotic heart disease, specifically defining acyanotic heart defects as congenital disorders with left to right shunting and obstructive lesions that are not always apparent at birth. It provides details on atrial septal defects (ASD) and ventricular septal defects (VSD), including their incidence, pathophysiology, clinical manifestations, diagnostic testing, and treatment options. The objectives are to define acyanotic heart defects, describe different types of defects, and discuss their etiology, clinical presentation, diagnosis, management, and relevant nursing care.

















































































