Downloaded 24 times


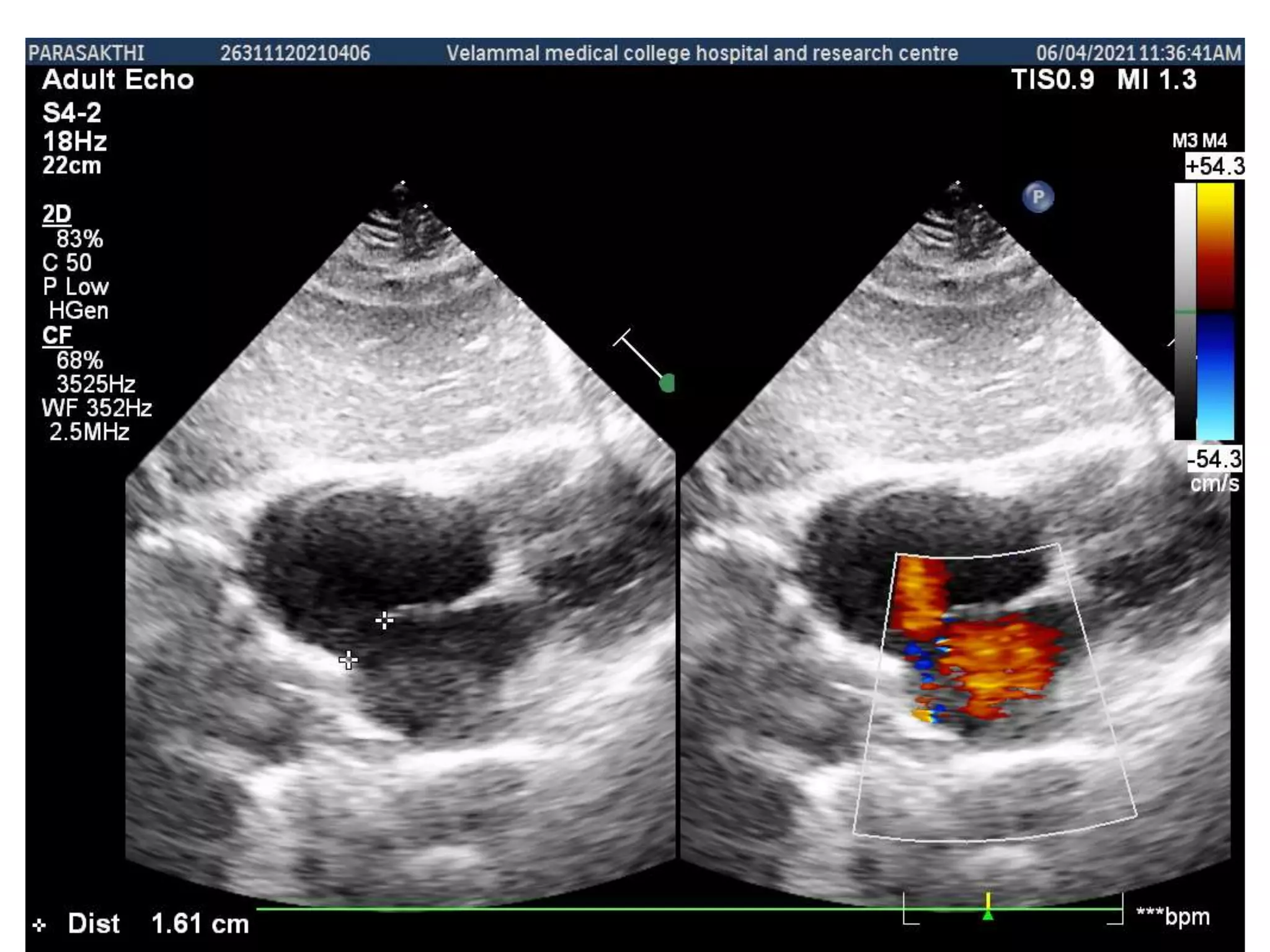

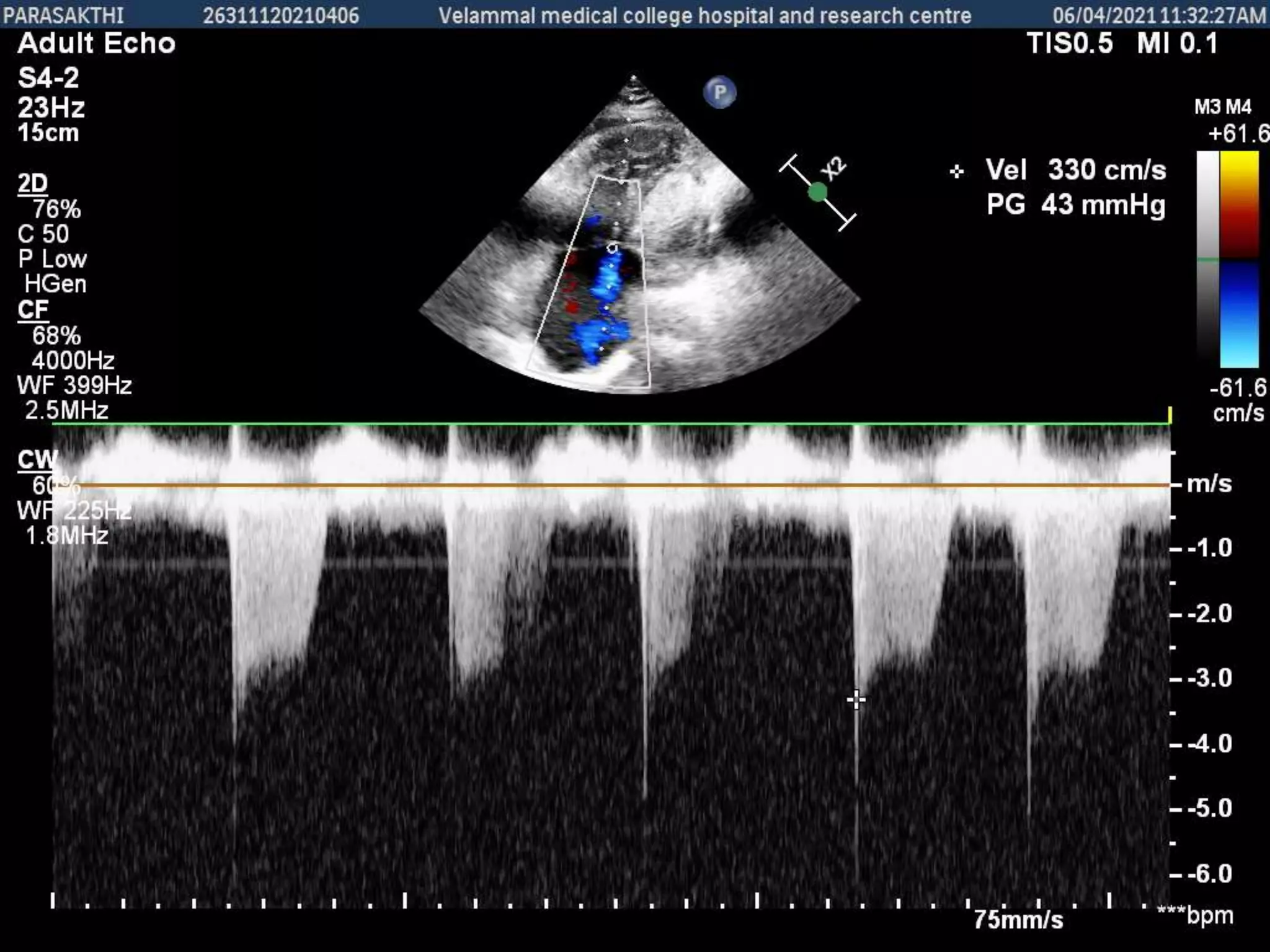
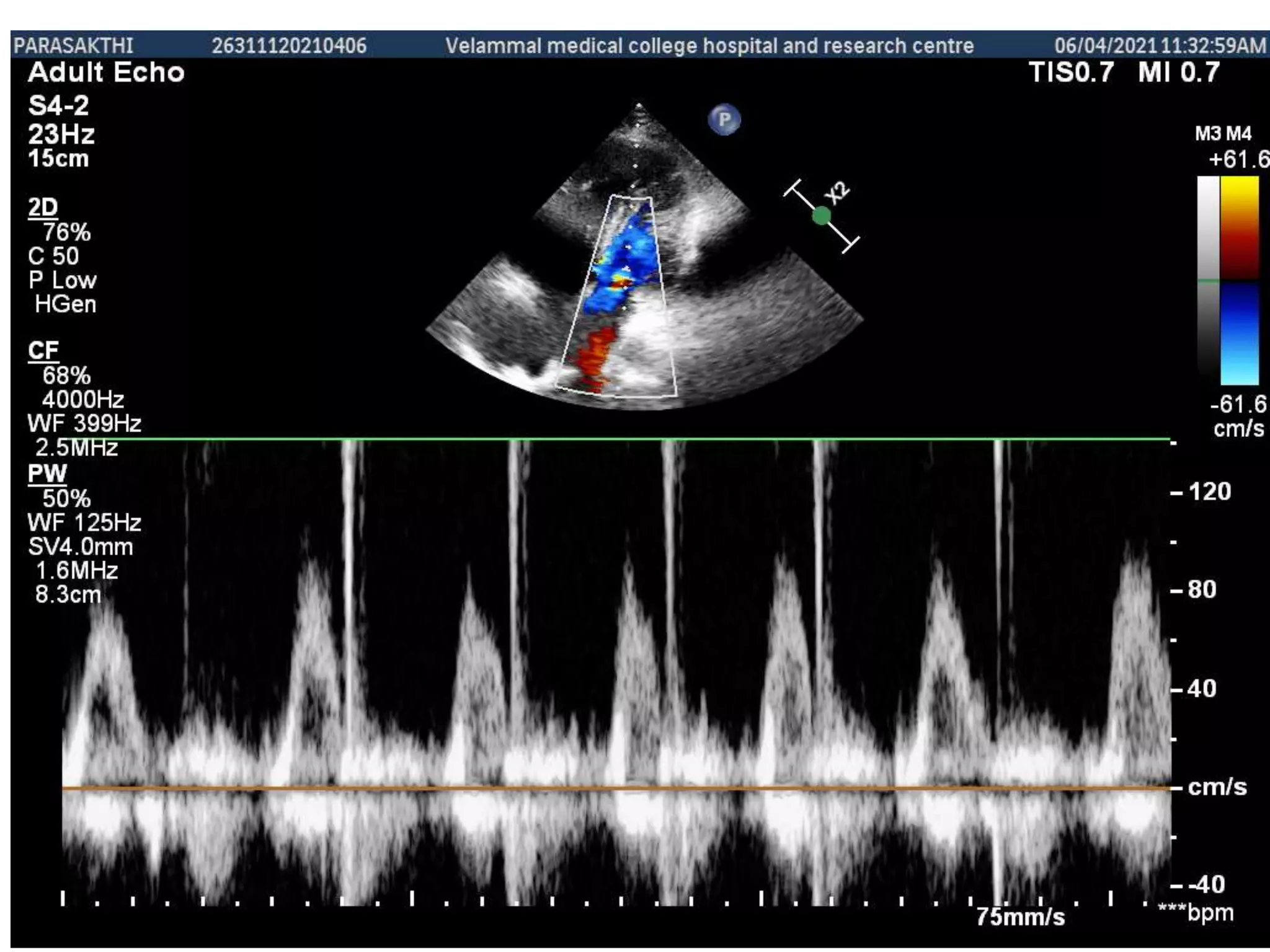


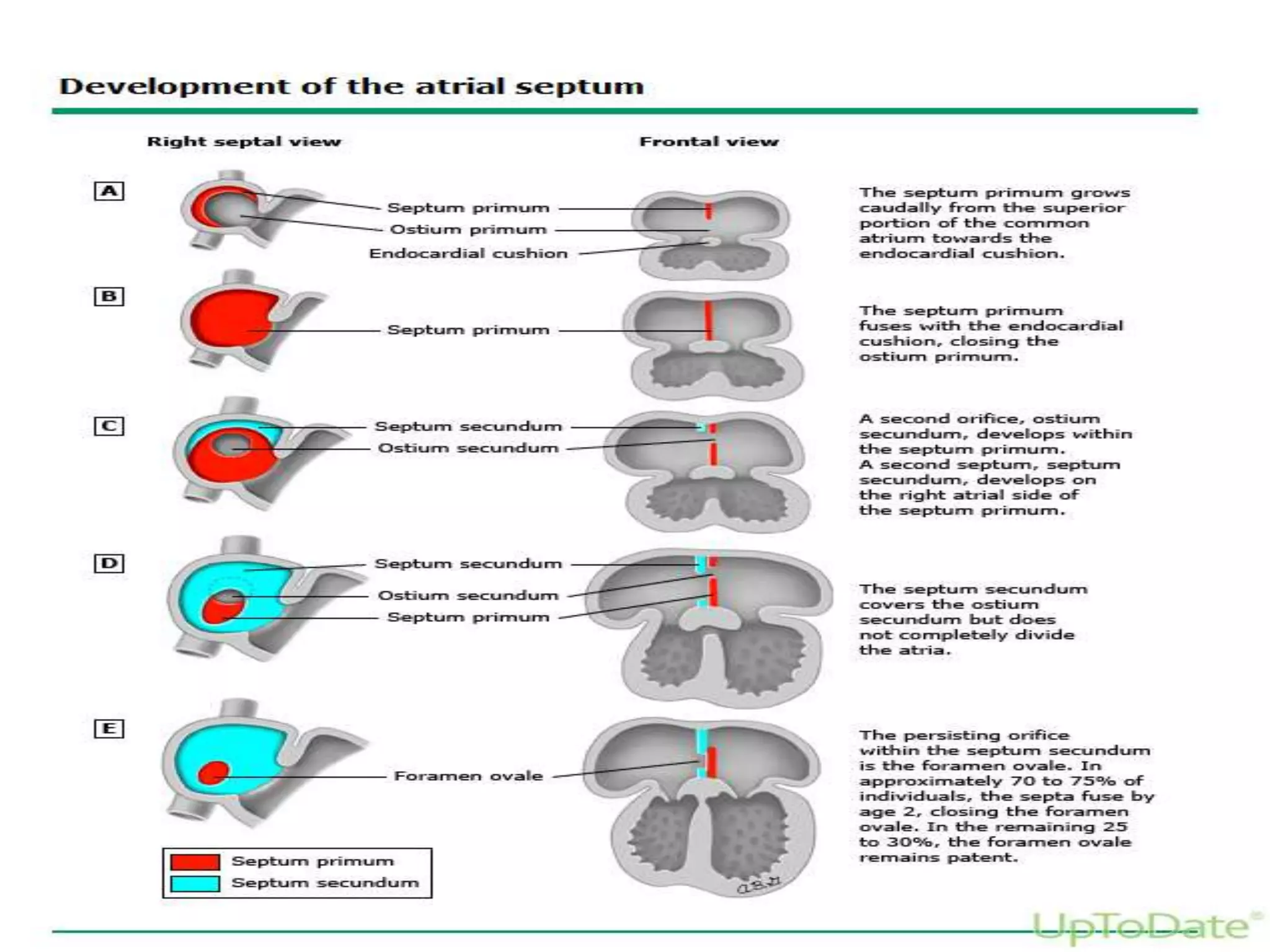
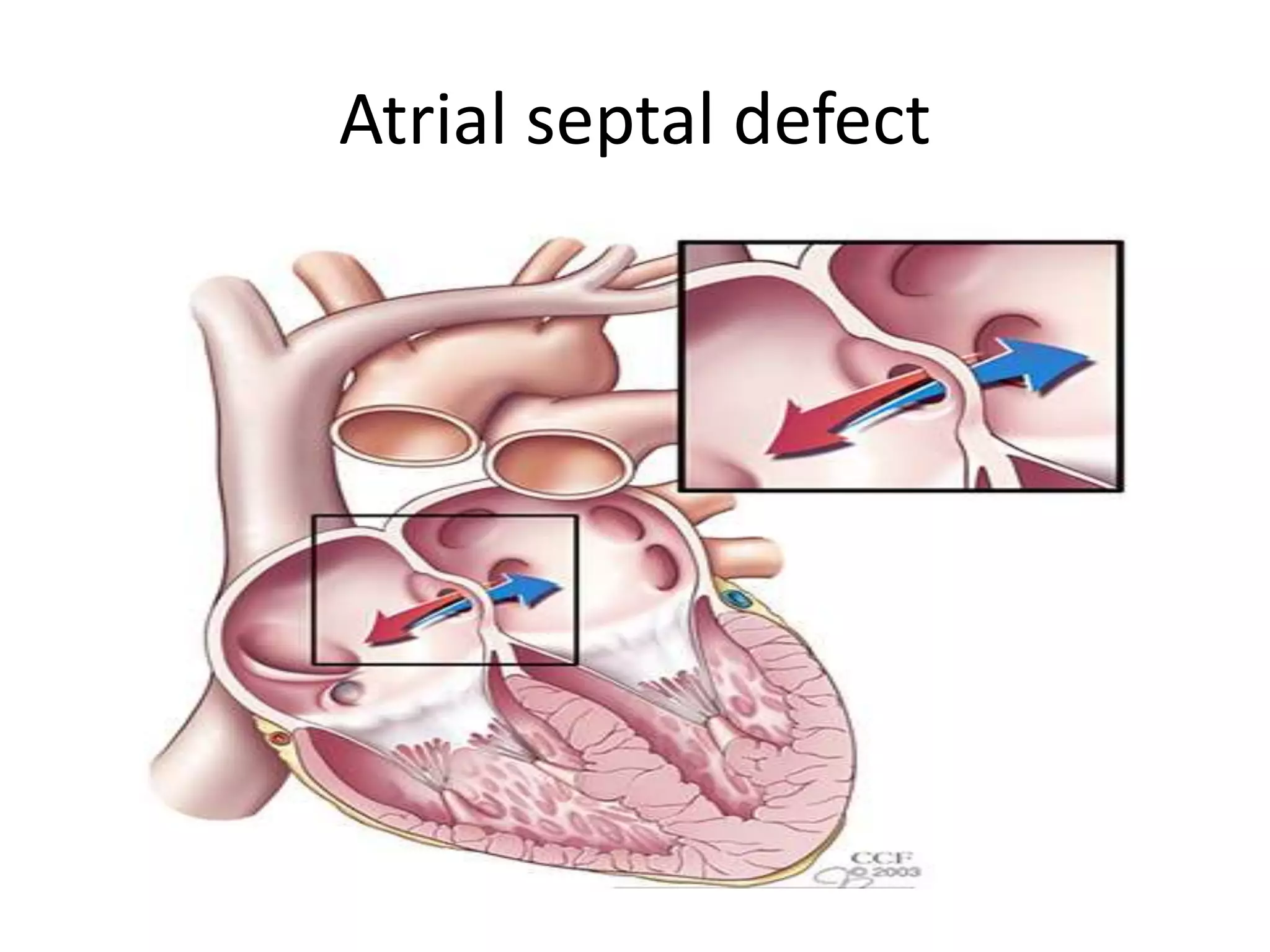



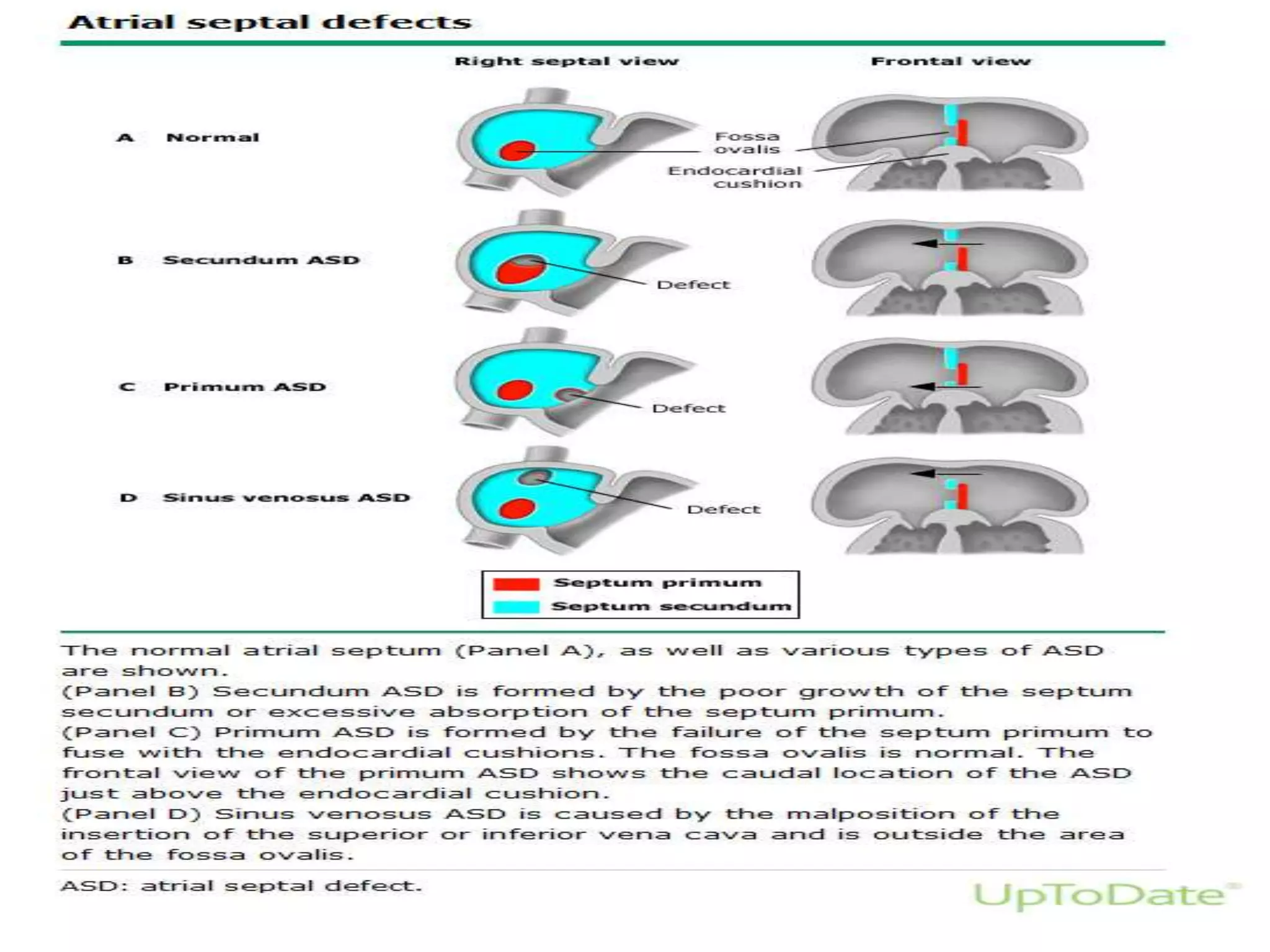
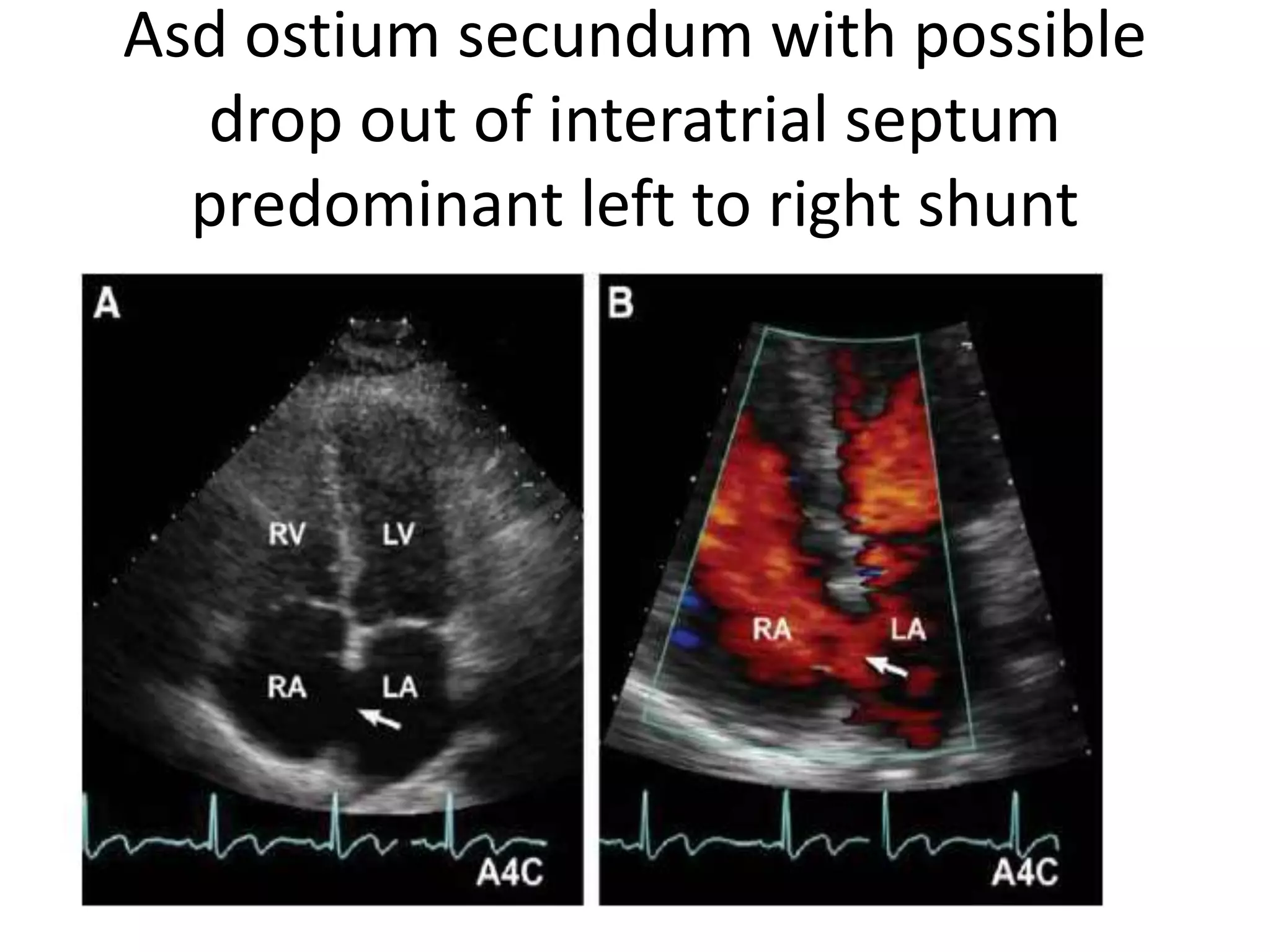







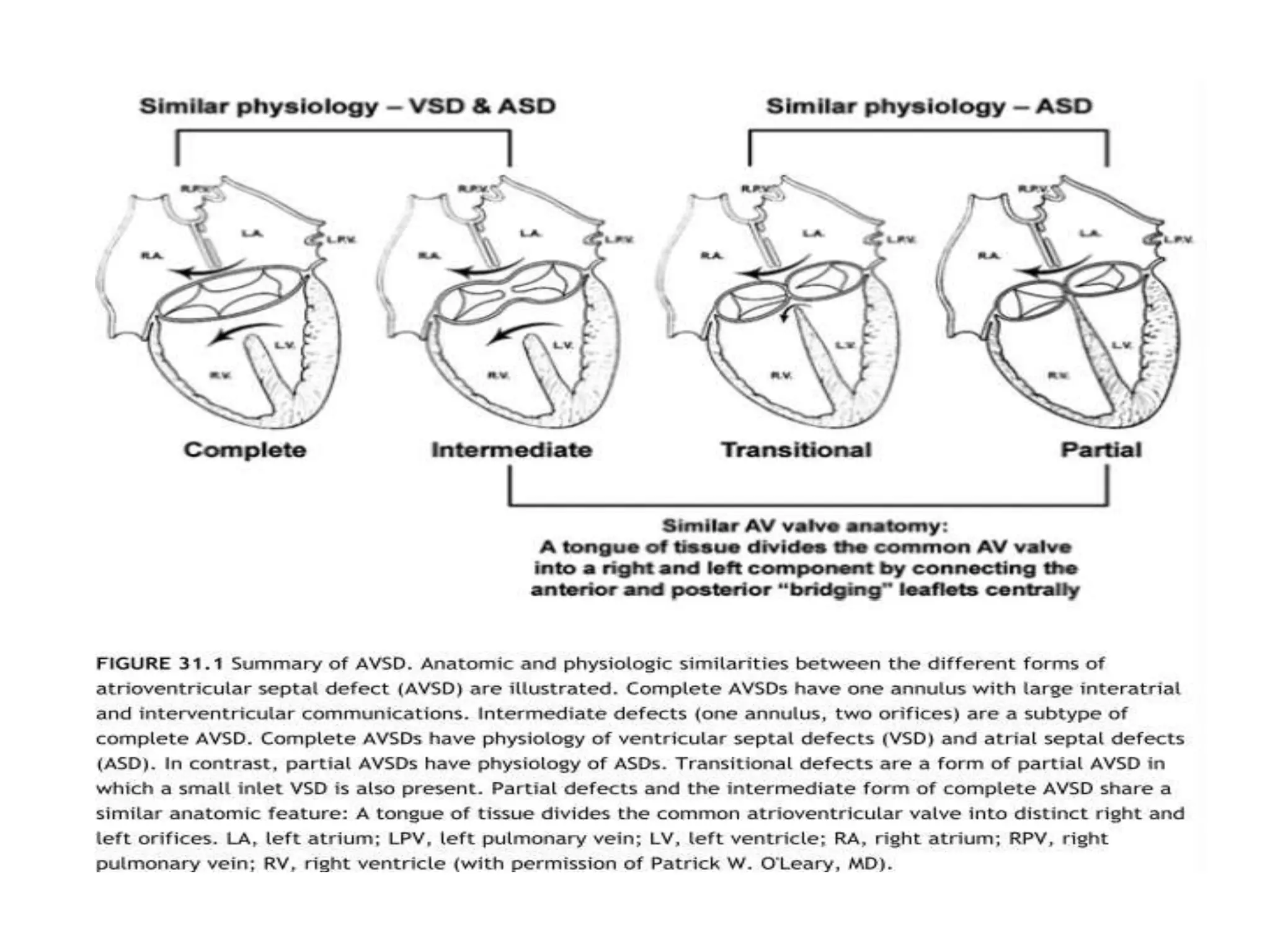


















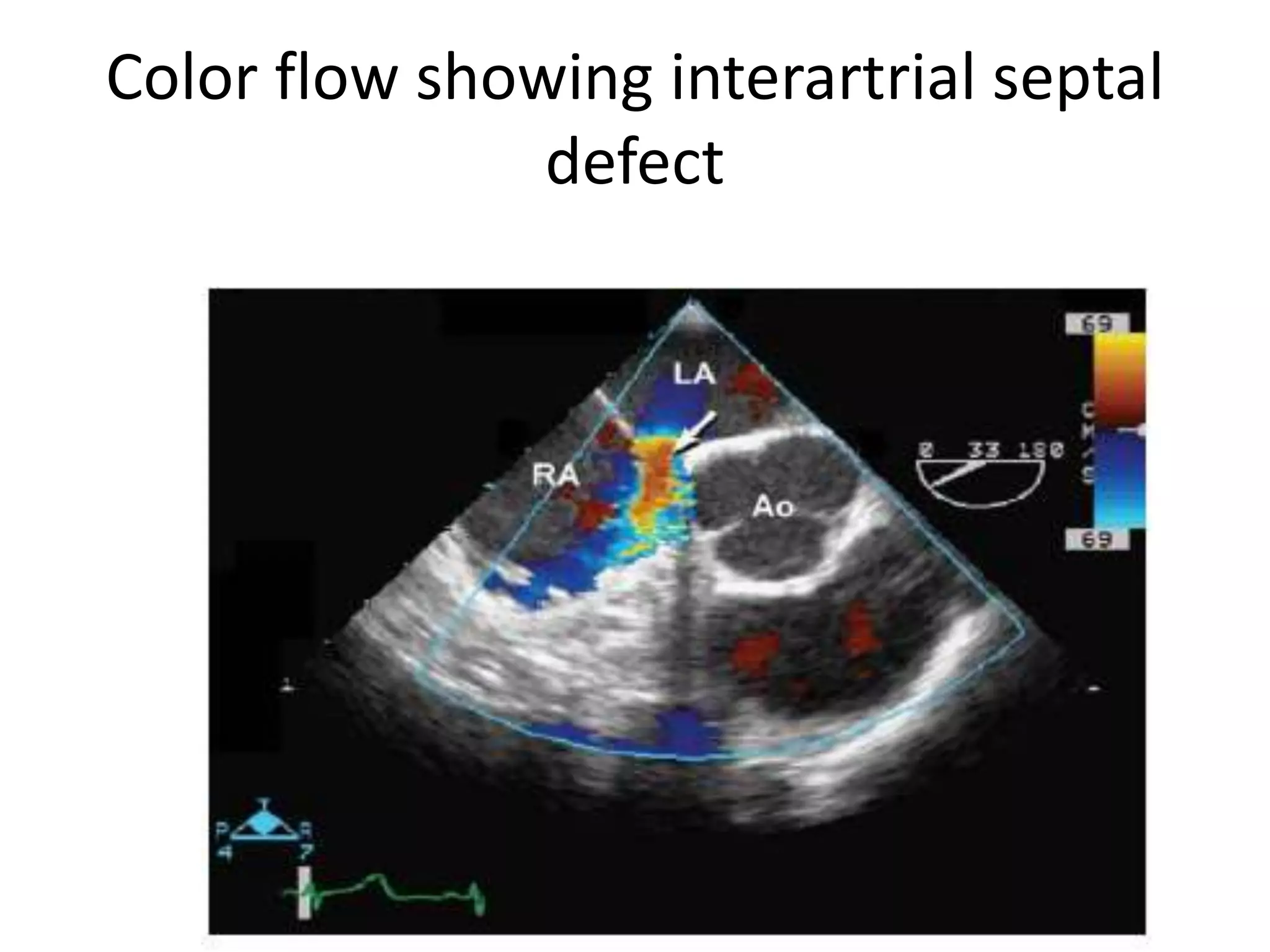











A 45 year old woman presented with shortness of breath on exertion. Echocardiography showed an atrial septal defect (ASD). ASDs are congenital heart defects where the wall separating the left and right atria is incomplete. The most common type is secundum ASD, which accounts for 70-75% of cases. ASDs allow blood to shunt from the left to the right atrium, overloading the right heart and lungs over time if not repaired. Echocardiography is the primary test to diagnose ASDs.




















































![ivct and ivrt IN CARDIAC CYCLE [Autosaved] .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ivctandivrtautosaved-copy-250829033609-78e4fe1b-thumbnail.jpg?width=640&height=640&fit=bounds)


































