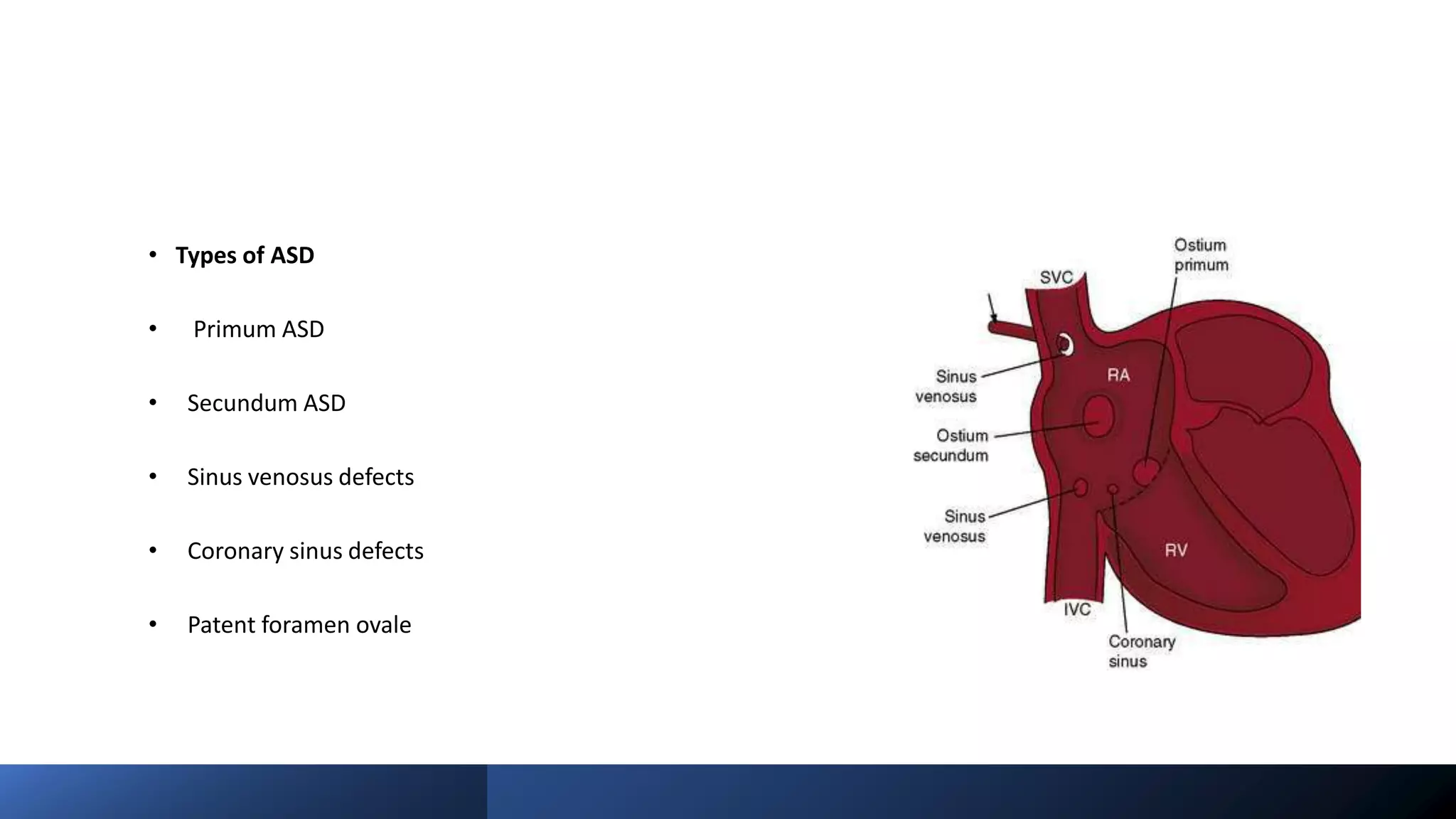
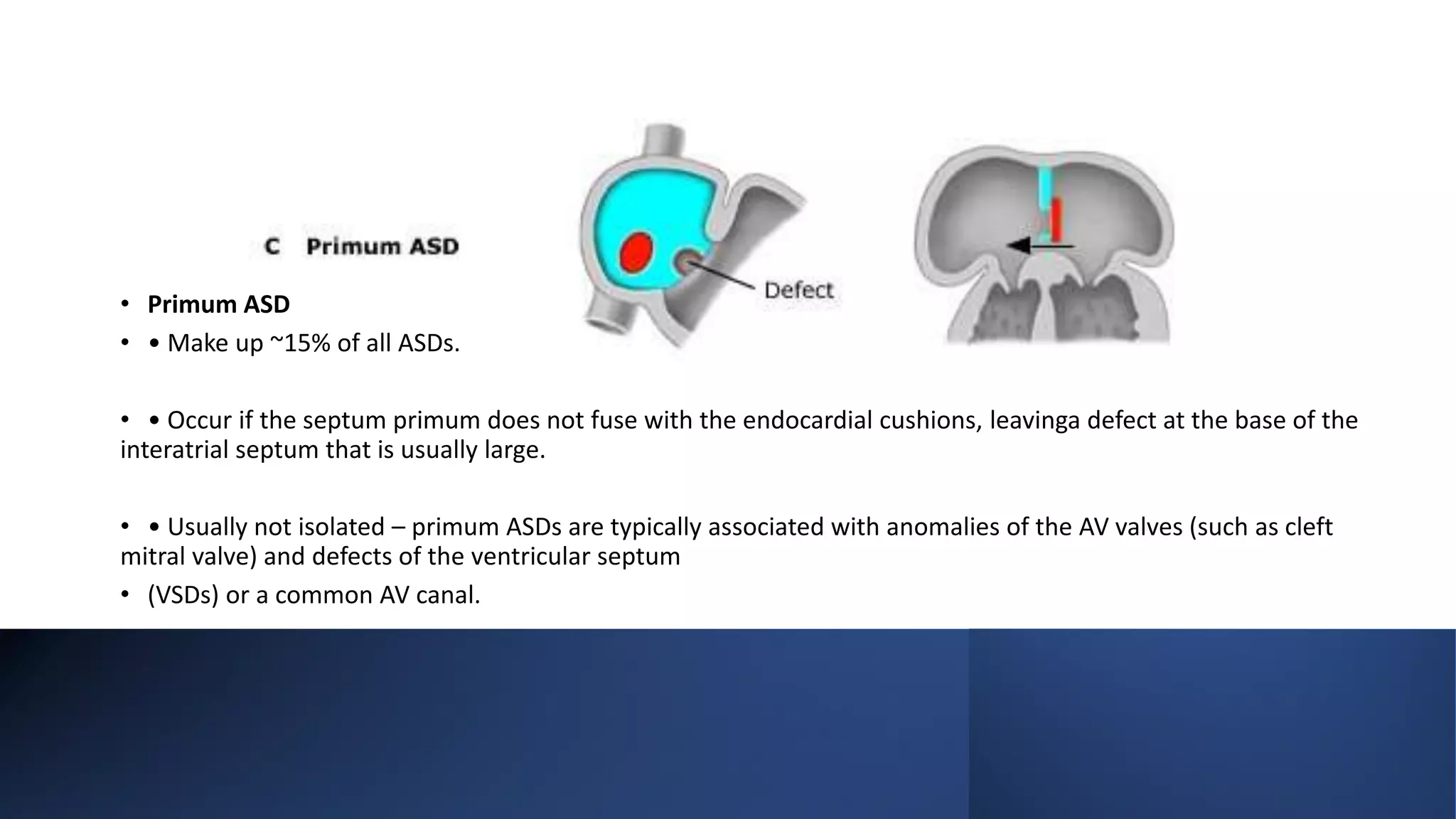
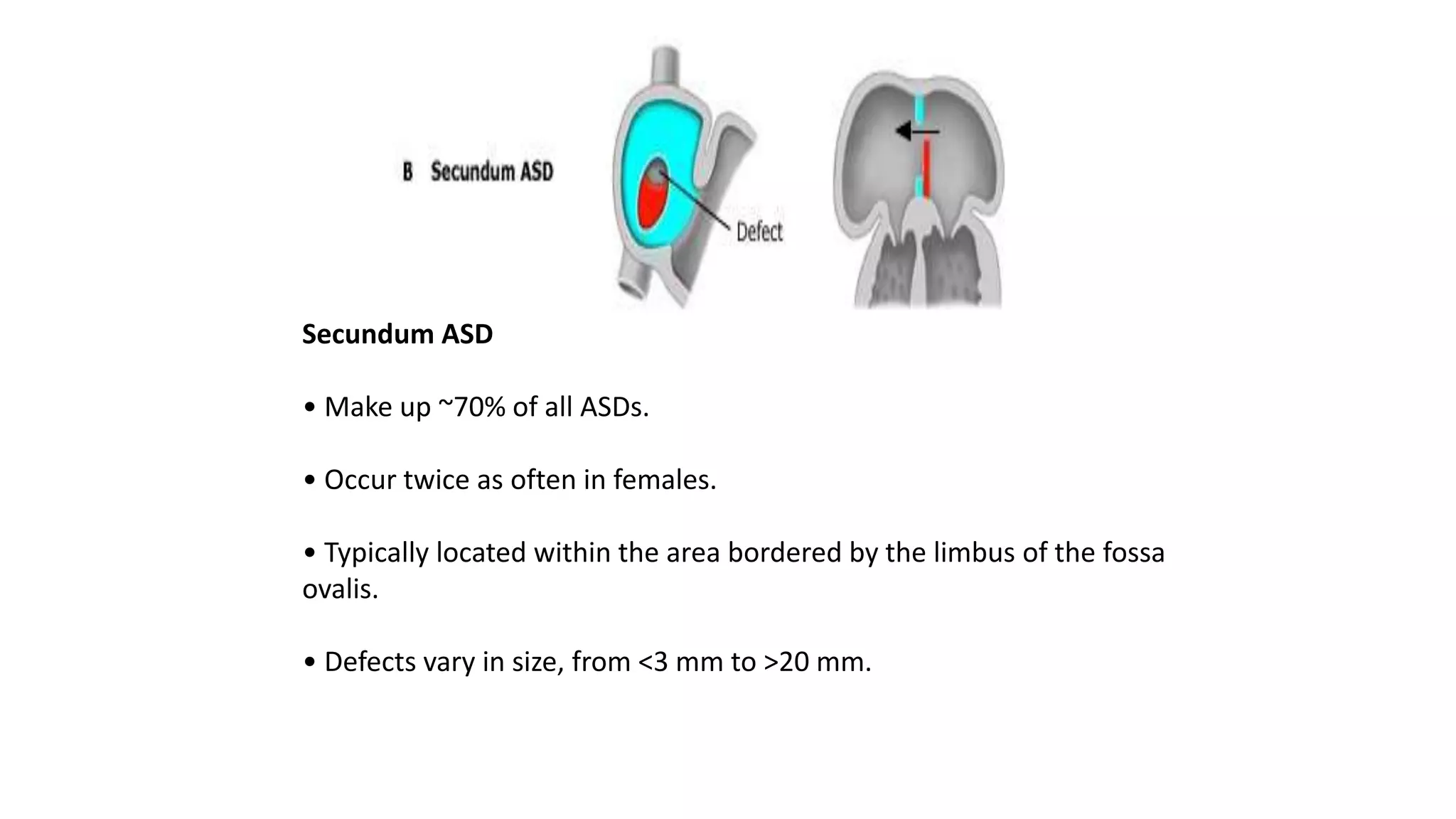
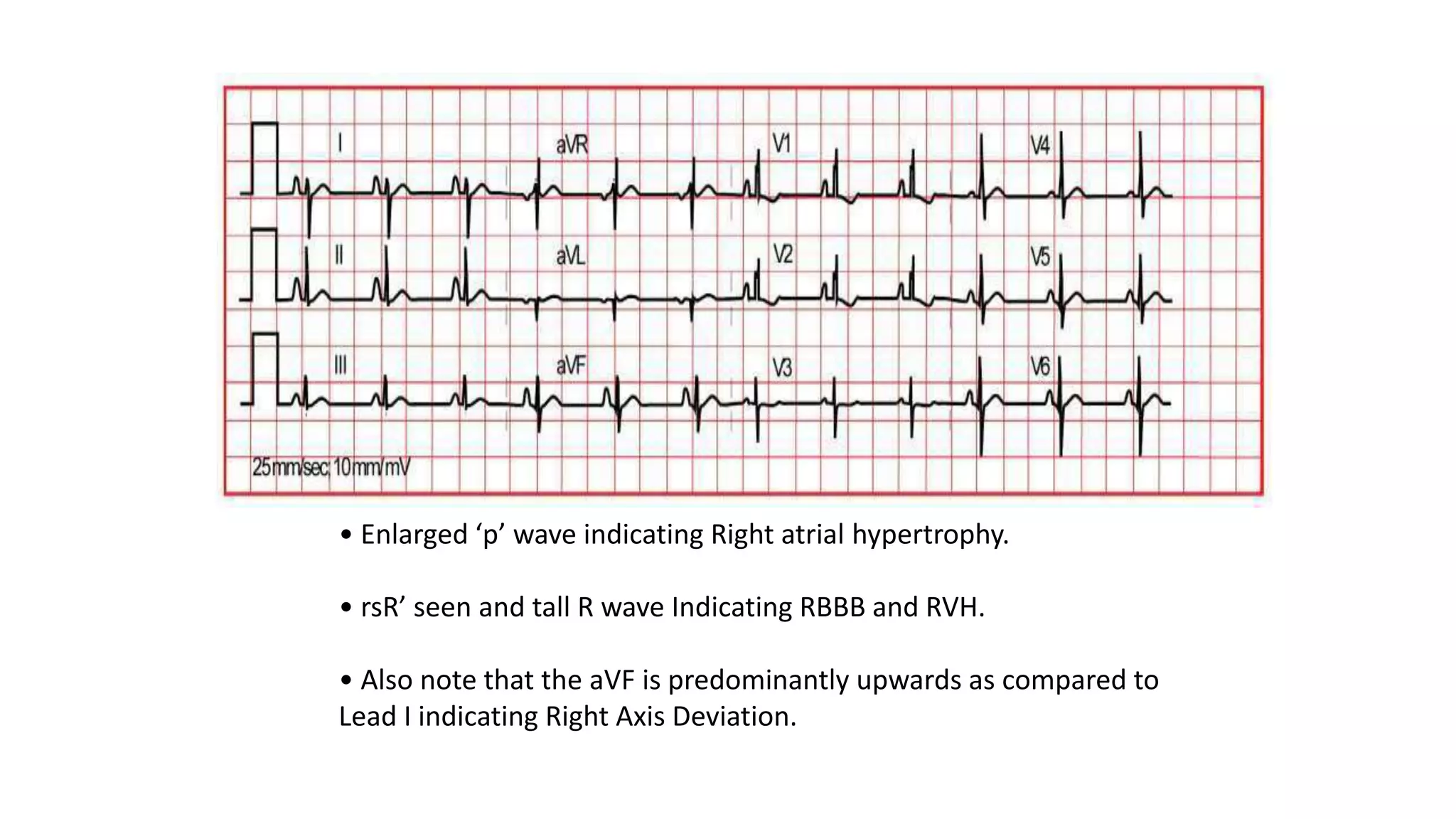
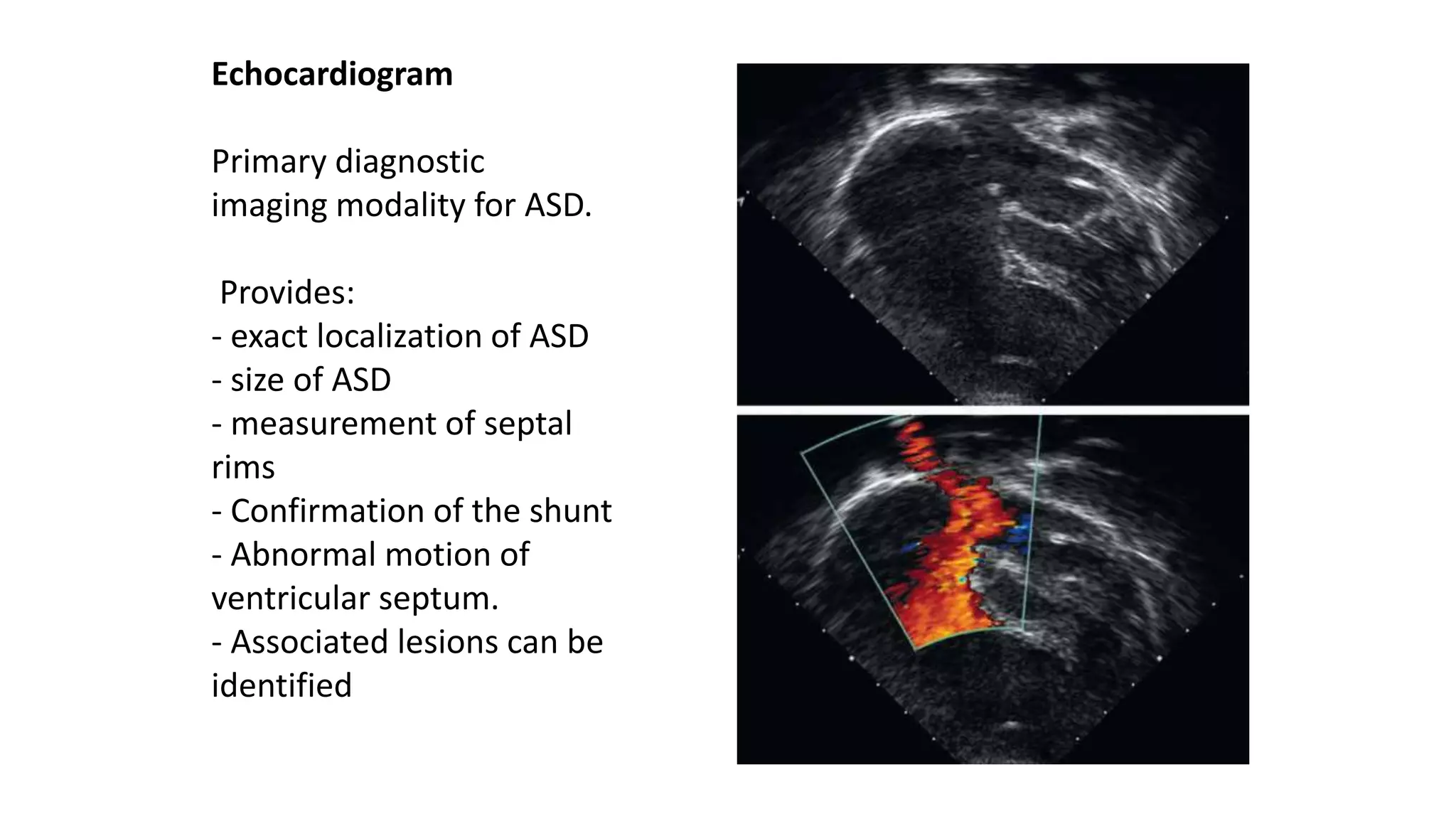
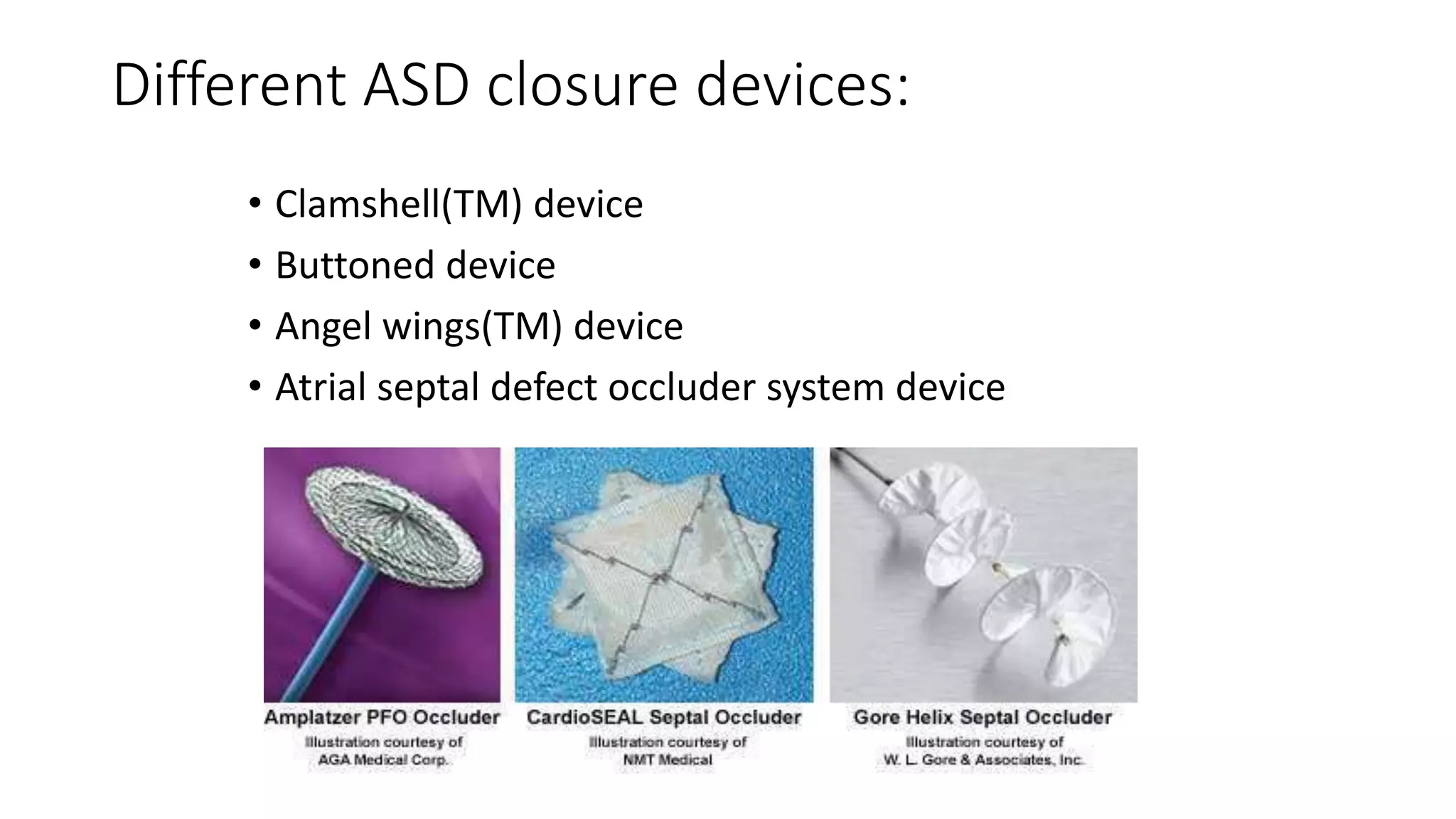
Atrial Septal Defect (ASD) is a congenital heart defect characterized by a hole in the atrial septum, occurring in 1 in 1500 live births and comprising 5-10% of congenital heart defects. It can manifest in various forms, primarily primum and secundum types, with differing implications for cardiac function and associations with other anomalies. Management options include medical therapy, interventional closures, and surgical repair, with the prognosis being generally favorable for early diagnosed and treated cases.