Downloaded 1,055 times








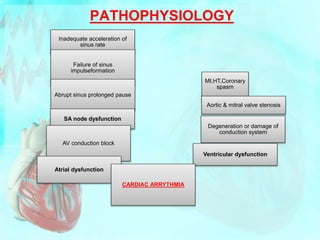

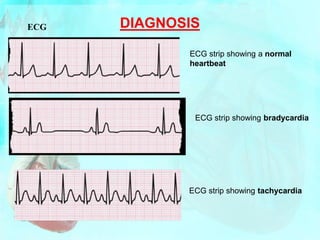





Arrhythmias are abnormalities in heart rate or rhythm that arise from problems with the heart's electrical system. They can be caused by issues with impulse formation or conduction. Arrhythmias are classified as tachyarrhythmias, which involve fast heart rates, or bradyarrhythmias, which involve slow heart rates. Common arrhythmias include atrial fibrillation, atrial flutter, and various types of heart block. Diagnosis involves electrocardiography and other cardiac tests. Treatment may involve medications, cardiac ablation, implanted devices, or surgery depending on the type of arrhythmia.
























































![Dysrhythmia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysrhythmiaautosaved-230617180733-e317f7a6-thumbnail.jpg?width=640&height=640&fit=bounds)







![ECG [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/ecgcompatibilitymode-230828072404-d338c45c-thumbnail.jpg?width=640&height=640&fit=bounds)