Downloaded 199 times
![Asthma Pathophysiology [email_address]](https://image.slidesharecdn.com/asthma-pathophysiologyn-1233730055155655-1-090616033540-phpapp02/85/Asthma-Pathophysiologyn-1233730055155655-1-1-320.jpg)
![Asthma Pathophysiology [email_address]](https://image.slidesharecdn.com/asthma-pathophysiologyn-1233730055155655-1-090616033540-phpapp02/75/Asthma-Pathophysiologyn-1233730055155655-1-1-2048.jpg)
![THANK YOU [email_address] 06/16/09](https://image.slidesharecdn.com/asthma-pathophysiologyn-1233730055155655-1-090616033540-phpapp02/85/Asthma-Pathophysiologyn-1233730055155655-1-30-320.jpg)

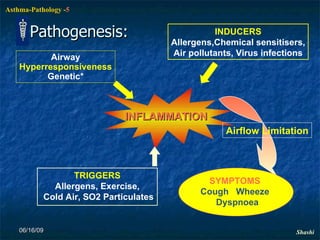
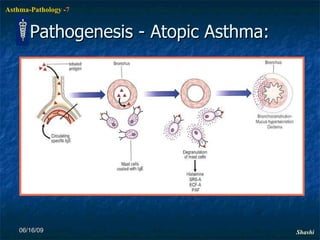
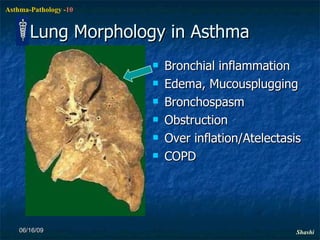
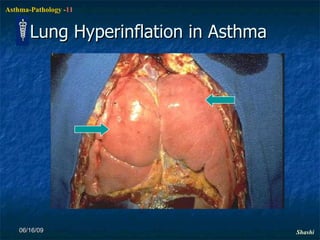
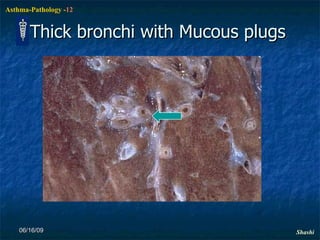
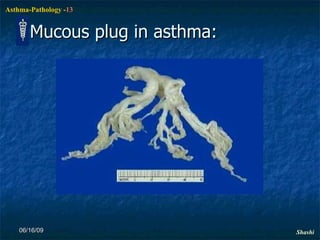
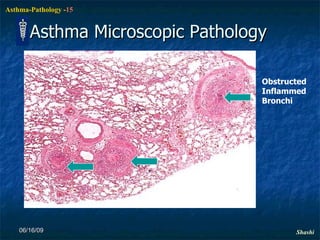
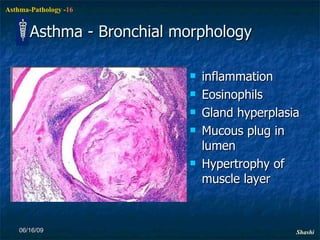
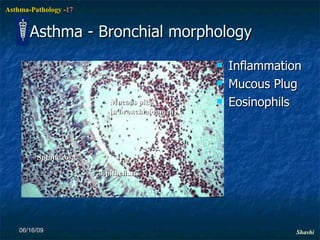
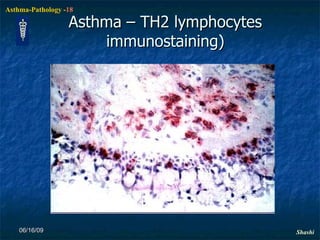
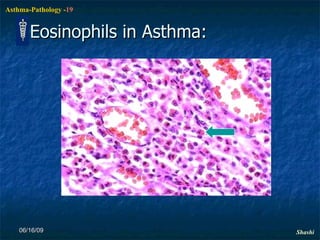
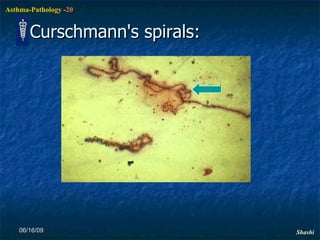
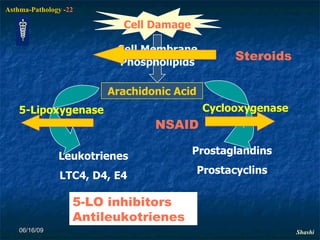
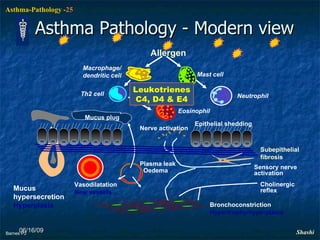
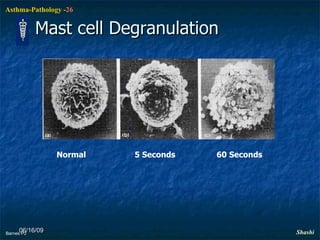
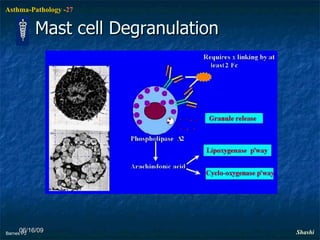
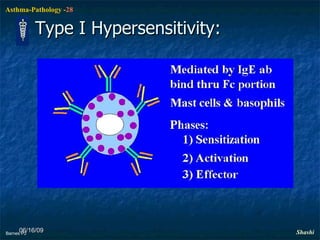
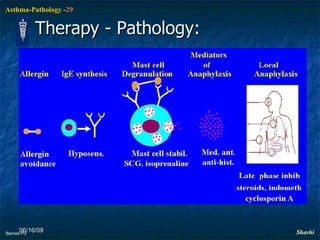
Asthma is a chronic inflammatory disorder of the bronchi characterized by episodic and reversible bronchospasm resulting from an exaggerated response to various stimuli like allergens. It affects around 10% of children and 5-7% of adults globally. The pathogenesis involves inflammation, airflow limitation, and airway hyperresponsiveness triggered by allergens, exercise, cold air, and other factors. Pathologically, asthma is associated with bronchial inflammation, edema, mucus plugging, and bronchospasm.























































































