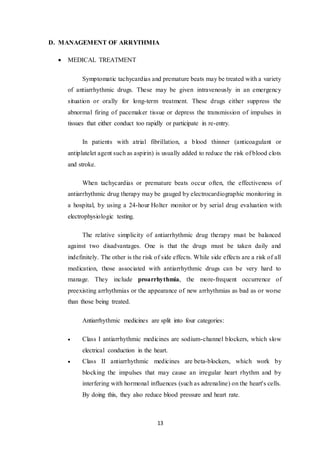
The document provides an overview of arrhythmias, which are changes from the normal sequence of electrical impulses in the heart that can result in irregular heartbeats. It discusses various types, classifications, causes, risk factors, and treatment options, including medications and procedures. Key factors influencing arrhythmias include coronary heart disease, high blood pressure, and lifestyle choices such as alcohol consumption and stress.












































![Mahkamah Agung [MA] - PKN SMPN49](https://cdn.slidesharecdn.com/ss_thumbnails/mahkamahagungma2-150327084851-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Bioteknologi - Membuat Roti [Biologi SMPN49]](https://cdn.slidesharecdn.com/ss_thumbnails/bioteknologi-150327094115-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)


![PKN - Konferensi Asia Afrika [KAA] (Annisa H, Safira Y, Siti Afifah R) 26-06-...](https://cdn.slidesharecdn.com/ss_thumbnails/pkn-konferensiasiaafrikaannisahsafiraysitiafifahr26-06-2013-150327100151-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Physics - Sound [SMPN49]](https://cdn.slidesharecdn.com/ss_thumbnails/soundpresentation-150327091731-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Drug-induced Toxicity [Liver, Kidney, Nervous System, Muscle]](https://cdn.slidesharecdn.com/ss_thumbnails/groupbgroup4drug-inducedtoxicity-151107045834-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![Fungsi Menu dan Icon Microsoft Publisher [ICT SMPN49]](https://cdn.slidesharecdn.com/ss_thumbnails/menudaniconpublisher-150327095123-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)


![[IMMUNOLOGY LAB REPORT] Antigen - Antibody Precipitation Reaction](https://cdn.slidesharecdn.com/ss_thumbnails/ouchterlonyannisaii-151107074605-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

![[Paperwork] Mixing - Pharmaceutical Engineering](https://cdn.slidesharecdn.com/ss_thumbnails/papermixingcomplete-151107042824-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Power Point] Mixing - Pharmaceutical Engineering](https://cdn.slidesharecdn.com/ss_thumbnails/forslideshare-151107043333-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)















![Dysrhythmia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysrhythmiaautosaved-230617180733-e317f7a6-thumbnail.jpg?width=640&height=640&fit=bounds)





![Shadechapter09.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter09-150421103043-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)







![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











