Downloaded 172 times










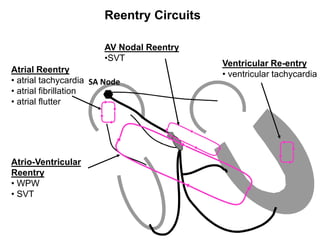

































































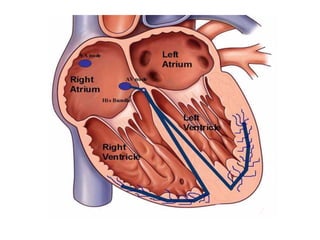































The document provides an overview of various cardiac arrhythmias, their mechanisms, causes, clinical manifestations, and treatments, focusing on specific types such as bradycardia, tachycardia, atrial fibrillation, and heart blocks. It also includes details on the electrical conduction system of the heart as well as specific ECG characteristics associated with each arrhythmia. Additionally, it highlights the importance of understanding these conditions for effective patient management and treatment.























































![ECG [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/ecgcompatibilitymode-230828072404-d338c45c-thumbnail.jpg?width=640&height=640&fit=bounds)






















