Downloaded 184 times
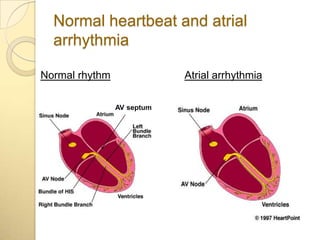
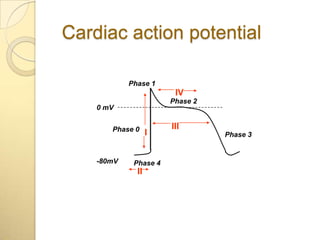
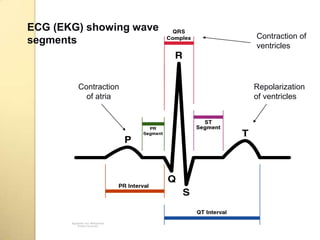
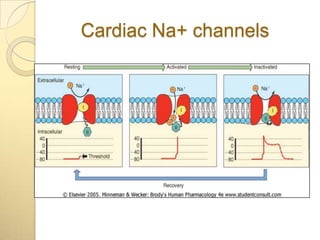
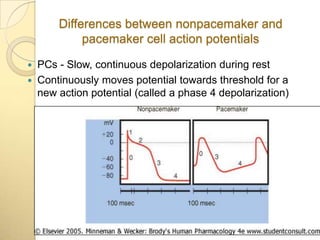
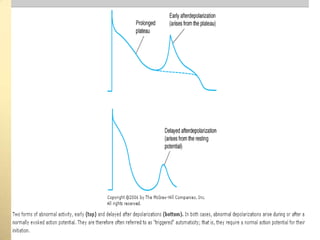
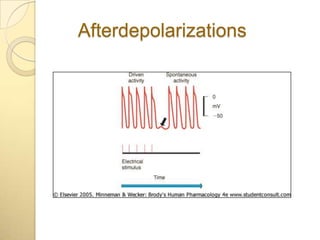
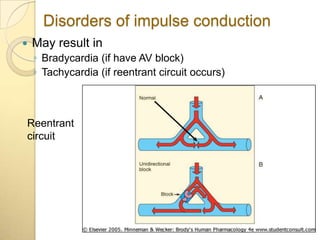

This document discusses cardiac arrhythmias and their treatment. It defines normal cardiac rhythm and atrial arrhythmias. It describes the cardiac action potential and ECG waves. It explains the differences between pacemaker and non-pacemaker cell action potentials. The document discusses mechanisms of arrhythmias including disorders of impulse formation and conduction. It provides an overview of antiarrhythmic drug classes and mechanisms of action including sodium channel blockade, beta-blockade, and calcium channel blockade.









































![Cardiology cases[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cardiologycases1-110707062202-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

































































